#2 Lecture Outline
I. Introduction
A. The emergency medical services (EMS) system is always evolving.
1. Originally, its primary role was transportation.
2. As awareness of EMS capabilities grew, the need for improved systems in various (primarily rural) locations became evident.
3. This awareness, along with research and guidelines from national organizations, has led to the advancement of EMS.
#3 Lecture Outline
4. The public’s perception of you is based on media exposure and personal experiences.
Treat all people with respect and dignity.
Continued education is a must.
#4 Lecture Outline
II. EMS System Development
A. Visionary advances
1. Much of the prehospital emergency medical care you will deliver as a paramedic can be attributed to the visionary advances of pioneers in the field including Drs. Peter Safar and Nancy Caroline.
#5 Lecture Outline
B. The history of EMS
1. 1487: The first use of an ambulance occurred during the Siege of Málaga.
a. Transport only
2. 1800s: Baron Dominique-Jean Larrey, chief physician in Napoleon’s army, is credited with establishing the first prehospital system for triaging and transporting patients.
3. 1865: The first civilian ambulance was used in Cincinnati, Ohio.
4. 1869: The first ambulance service started at the Bellevue Hospital in New York City.
5. 1899: The first operated automobile-type ambulance was used at the Michael Reese Hospital in Chicago, Illinois.
6. A major shift occurred between World War I and World War II.
a. Many hospital-based ambulance services did not survive.
7. 1926: The Phoenix fire department started service similar to present-day EMS.
8. 1928: Julian Stanley Wise launched the first rescue squad in Roanoke, Virginia.
a. Soon after, numerous other rescue squad organizations were developed along the East Coast, primarily in New Jersey.
9. 1940s: EMS was turned over to fire and police departments due to lack of personnel.
No minimum standard of training was set.
The role of providing care was not always accepted or welcomed.
#6 Lecture Outline
C. The 20th century and modern technology
1. During World War I and World War II, systems for field treatment and transport (battlefield corps) continuously evolved.
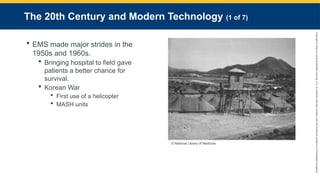
2. EMS made major strides in the 1950s and 1960s.
3. Military medical researchers recognized bringing hospital-type services closer to the field gave patients a better chance of survival.
a. Helicopters were first used in 1951 during the Korean War.
b. MASH units
#7 Lecture Outline
4. 1956: Mouth-to-mouth resuscitation was developed by Drs. Elan and Safar.
a. The portable defibrillator was developed by Frank Pantridge in 1959.
5. Late 1950s/early 1960s:
a. Focus moved back to bringing the hospital to the patient.
b. Mobile intensive care units (MICUs) were developed.
#8 Lecture Outline
6. 1965: The National Academy of Sciences and the National Research Council released “The White Paper.”
a. Also called “Accidental Death and Disability: The Neglected Disease of Modern Society”
b. Findings included:
i. A lack of uniform laws and standards
ii. Ambulances and equipment of poor quality or nonexistent
iii. Lack of communication between EMS and hospitals
iv. Lack of personnel training
v. Hospitals staff only part time
vi. More people died in motor vehicle crashes than in the Vietnam War
#9 Lecture Outline
7. Findings outlined 10 critical points to establish a functioning system.
a. Led to the National Highway Safety Act
b. Created the US Department of Transportation (US DOT)
8. 1968: Task Force of the Committee of EMS created basic training standards and principles of a 9-1-1 system to provide universal access to emergency services.
a. Refer to Table 1-1 for the critical points, required components, and system elements of EMS developed as a result of “The White Paper.”
#10 Lecture Outline
9. 1969: Dr. Eugene Nagel of Miami, Florida, created the first true paramedic program.
a. Trained firefighters with advanced emergency skills
b. Developed a telemetry system
c. Often called the Father of Paramedicine
d. Standards for ambulance design and equipment were published this year.
10. 1970s:
a. Helicopters for medical transport became available.
b. The National Registry of Emergency Medical Technicians (NREMT) was established.
#11 Lecture Outline
11. 1971:
a. Emergency Care and Transportation of the Sick and Injured was published.
b. AAOS began training EMTs through a national workshop.
c. Emergency!, the first television program focused on EMS, began an 8-year run.
12. 1973: The Emergency Medical Services Systems Act was passed.
a. Defined 15 required components of an EMS system
i. Refer to Table 1-1
b. Emphasis on regional development and trauma care
c. Provided a structure and uniformity to the EMS system that came out of pioneering programs in Miami, Seattle, and Pittsburgh, and the Illinois Trauma System (Dr. David Boyd)
13. 1974:
a. Federal report disclosed fewer than one-half of ambulance personnel completed sufficient training.
b. Guidelines published for development and implementation of EMS systems
14. 1975:
a. The American Medical Association recognized emergency medicine as its own branch within medicine.
b. Many cities set up individual advanced EMS training.
15. 1977: The first National Standard Curriculum for paramedics was developed by the US DOT.
#12 Lecture Outline
16. 1980s/1990s:
a. The number of trained personnel grew significantly.
b. The National Highway Traffic Safety Administration (NHTSA) developed 10 system elements to help sustain an EMS system.
c. Federal funding and staff for EMS were reduced.
d. Responsibility for EMS was transferred to the states.
e. Funding continues to be a significant challenge for states and local governments.
f. Major legislative initiatives:
i. EMS for Children (EMSC) program implemented in 1985
ii. Amendment to the Public Safety Officers’ Benefit Program in 1986
g. Trauma systems started making headway in the 1990s.
#13 Lecture Outline
D. The 21st Century
1. Numerous initiatives are appearing.
a. The National EMS Quality Alliance (NEMSQA; formerly called EMS Compass) is an organization measuring performance for EMS and health care partners.
b. EMS training is being used in many other areas of health care.
c. Community paramedicine, the health care model in which experienced paramedics receive advanced training to provide additional services, is making continuing strides.
2. These additional capabilities are not being developed to replace current health care modalities, but rather to apply the capabilities of paramedics in areas not served previously.
#14 Lecture Outline
III. Licensure, Certification, and Registration
A. Registration means that records of a paramedic’s education, state or local licensure, and recertification will be held by a recognized board of registration.
1. Depending on your state or location, you may be licensed or registered.
2. Once you complete your initial paramedic education, depending on your state, you will be eligible to take your state’s certification examination.
3. Some states require you to test and establish licensure through a registry system such as the NREMT.
B. A certification examination is used to ensure that all health care providers have the same basic level of knowledge and skill.
1. Once you have passed the required examinations, your state and/or NREMT will give you a certificate or license.
C. Licensure is how states control who is allowed to practice as a health care provider.
1. Depending on the state, this may be known as licensure, certification, or credentialing.
2. Performing functions as a paramedic before licensure is unlawful.
3. State, local, and national agencies require that paramedics receive medical direction.
4. If your state requires you to pass the NREMT cognitive and psychomotor examinations to become licensed, you will have to pass a written exam and demonstrate several practical skills.
a. To be eligible, you must successfully complete initial paramedic education through an accredited program.
b. The National Registry exam tests to the Paramedic Psychomotor Competency Portfolio, a comprehensive collection of skills and scenarios.
#15 Lecture Outline
D. The Committee on Accreditation of Educational Programs for EMS Professions (CoAEMSP) is currently the only accrediting body for paramedic programs.
1. Its mission is to continuously improve the EMS education quality through accreditation and recognition services.
2. The number of paramedic training facilities will grow significantly over the coming years.
#16 Lecture Outline
E. Reciprocity addresses training that occurred in a place other than where a paramedic wants to practice.
1. Each state has different licensing or certification requirements and procedures.
2. Reciprocity: when certification is granted to a provider from another state or agency
3. Investigate the licensure process beforehand if you are planning to relocate to another state or country.
a. Many countries will not accept the training provided in the United States, and reciprocity will not be automatic.
b. Many states recognize National Registry certification as part of their reciprocity process.
c. Individual states may have specific requirements that must be met before reciprocity is granted.
#17 Lecture Outline
IV. Traditional EMS Employment
A. Once you become licensed, you will have a variety of different career options available to you.
1. Some career possibilities include the following:
a. Fire-based EMS (integrated into a fire department)
i. Most are paid and operated by the municipal government.
ii. Some locations operate fully with nonpaid volunteers while others use providers who are paid per call.
iii. EMS may have a separate management system and operate independently from the fire side.
iv. Fire departments can better justify keeping a staffed in-house department if they add EMS.
b. Third-service EMS (municipalities) (single or shared)
i. Depending on financial capability, some municipalities establish and operate their own ambulance services independent of fire, police, and other public safety entities.
ii. Independent ambulance agencies may also offer their services under contract to municipalities who cannot afford to provide their own services.
iii. Some states allow multiple municipalities to share services, with each being an equal owner.
iv. Usually, citizens need to request a response; they may not be sent automatically.
(a) The fire department would also have to request EMS response unless a prearranged process exists.
c. Private EMS agency (for-profit or nonprofit)
i. Operate similarly to third-service EMS agencies
ii. Contract services to municipalities
iii. Operations vary greatly
d. Hospital-based EMS
i. In most cases, hospital-based services tend to offer interfacility-type transports, as well as aeromedical services, which are offered in larger and remote organizations.
ii. Some also offer 9-1-1 response and paramedic intercept service.
iii. Paramedics are required to assist with patient care in other areas of the hospital in their down time.
iv. Typically, paramedics will function in an emergency department (ED), but they may be part of an internal emergency response team.
v. One benefit: access to information paramedics have from various medical providers.
e. Hybrid or other
i. Many large companies, such as those operating oil drilling platforms and factories with hundreds or thousands of employees have their own medical response and care facilities.
ii. In some areas, paramedics work in conjunction with other healthcare providers.
iii. There are numerous companies whose business is to hire personnel to fill medical positions at specific locations, such as national parks, amusement parks, and other venues.
#18 Lecture Outline
V. The EMS System
A. The EMS system is a complex network of coordinated services that provides various levels of care to the community.
1. These services work in unison to meet the needs of the community.
2. The EMS system begins with citizen involvement.
a. The public needs to be taught how to:
i. Recognize what is an emergency and what is not.
ii. Activate the EMS system.
iii. Provide basic care before EMS arrives.
#19 Lecture Outline
3. Factors that play a role in determining the outcome or likelihood of your patient’s survival include:
a. Bystander care
b. Dispatch (including prearrival directions)
c. Response (both mode and distance)
d. Prehospital assessment and care provided (level of EMS-trained personnel)
e. Transportation (ground ambulances, critical care units, air transport)
f. Emergency department care (on-duty trained emergency physicians and staff)
g. Definitive care (including trauma, pediatric, and neurologic specialists)
h. Rehabilitation
#20 Lecture Outline
4. The public’s first contact is usually a dispatcher.
a. Requirements for dispatcher training vary greatly from state to state.
b. Roles of the dispatcher
c. The scene may be different from what was relayed by the dispatcher.
5. As a paramedic you must:
a. Develop a care plan
b. Determine the most appropriate facility
#21 Lecture Outline
VI. Levels of Education
A. Federal to local level of EMS functioning
1. Federal level
a. NHTSA created the National EMS Scope of Practice Model.
2. State level
a. Licensure is usually a state function.
b. Laws and regulations are enacted to specify how EMS providers will operate.
c. Licensure is controlled by state-level EMS administrative offices.
d. Many states have a set of statutes or rules to be followed and a scope of practice for every EMS level.
e. The service’s medical director normally develops a set of patient care guidelines that outline the approved skills and treatments for each level.
3. Local level
a. Local medical director decides the day-to-day limits of EMS.
#22 Lecture Outline
4. Consistency as a result of national guidelines
a. The medical director can limit the scope of practice.
b. Expanding the scope of practice requires state approval.
5. 2009: The National Standard Curricula for all levels revised to the National EMS Education Standards
a. NHTSA: federal administrative source
b. Covers four levels of EMS providers
#23 Lecture Outline
B. The dispatcher
1. Plays a critical role
2. May be trained as an emergency medical dispatcher
3. May provide simple prearrival instructions (i.e., cardiopulmonary resuscitation [CPR], bleeding control) after asking a series of questions to a caller
#24 Lecture Outline
C. Emergency medical responder (EMR)
1. Until recently, the EMR was known as the “first responder.”
2. Not all states have this as a certification and/or licensing level.
3. An EMR is usually trained in CPR and/or first aid.
a. In some states, EMRs can function only as part of an organized group, and that group must be affiliated with a transporting ambulance service.
4. An EMR has completed a course covering the National EMS Education Standards for the EMR level.
5. EMRs should be able to:
a. Recognize the seriousness of a patient’s condition
b. Administer appropriate basic care
c. Relay information to the paramedic
6. EMRs are an essential level of provider to the EMS system, especially in rural areas.
#25 Lecture Outline
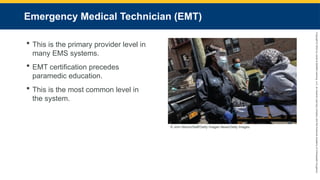
D. EMT
1. An EMT was formerly called EMT-Basic (EMT-B).
2. The EMT is the backbone and primary provider level in many EMS systems.
3. Providers must be EMT certified before entering a paramedic education program.
4. Skills and treatments vary from state to state. In some states, EMTs may be trained in:
a. Advanced airway intervention
b. Limited medication administration
c. Intravenous (IV) fluid therapy
5. Even if they have an expanded scope of practice, EMTs are not recognized with a different certification level per the National EMS Education Standards.
6. More providers are trained and certified at this level than at any other level in the EMS system.
#26 Lecture Outline
E. Advanced EMT (AEMT)
1. Formerly called EMT-Intermediate (EMT-I)
2. Initially developed in 1985
a. A major revision took place in 1999.
b. Recent changes to the National EMS Scope of Practice Model replace the intermediate EMT level with AEMT level in most states.
3. Trained in:
a. More advanced pathophysiology
b. Some advanced procedures, such as:
i. Establishing IV access
ii. Administering IV fluids
iii. Performing blood glucose monitoring
iv. Administering several medications
v. Performing some advanced airway management
#27 Lecture Outline
F. Paramedic
1. The paramedic is the highest EMS skill level to be certified or licensed at the national level.
a. Major revisions to the curriculum in 1998 increased level of training and skills greatly.
b. Starting in 2013, to test through NREMT, a paramedic student must have attended and successfully completed training at an accredited institution.
i. States that do not employ NREMT may not require EMS training institutions be accredited.
2. Even if one holds a license or is certified independently, states still require paramedics to:
a. Function directly under the guidance of a licensed physician
b. Be affiliated with a paramedic-level service
3. Some states allow paramedics to complete further education and earn the title of critical care paramedic.
a. This varies from state to state.
b. Research your state’s laws to see if this is allowed.
#28 Lecture Outline
VII. Paramedic Education
A. Initial education
1. Most states base paramedic education programs on the National EMS Education Standards.
a. As part of the 2009 revisions to the standards, inclusion of a college-level anatomy and physiology course was recommended as part of the training program.
i. Some training institutions offer this as part of a paramedic training program; others require it as a prerequisite.
b. The standards outline the minimum of what a paramedic must know to practice.
c. States require varying hours of education.
i. National average falls between 1,000 and 1,500 hours of combined classroom, clinical, and field education.
ii. Some leaders want to structure paramedic education so it is achieved through an accredited associate or bachelor’s degree program.
#29 Lecture Outline
B. Continuing education
1. Most states require paramedics to complete a certain number of continuing education hours and/or refresher programs.
2. Attend conferences and seminars whenever possible.
3. Keep up with reading EMS journals and research publications.
4. Consider continuing education organizations that are accredited through the Commission on Accreditation for Pre-Hospital Continuing Education (CAPCE).
a. Formerly called the Continuing Education Coordinating Board for EMS (CECBEMS)
b. Develops continuing education standards and is involved in setting accreditation standards for prehospital providers.
5. Get everyone in your service involved in postrun critiques.
6. Responsibility for continuing education ultimately rests with each individual paramedic.
#30 Lecture Outline
VIII. Additional Types of Transports
A. Transport to specialty centers
1. Many EMS systems include specialty centers focusing on specific types of care or specific types of patients.
2. Specialty centers normally have in-house specialists.
3. Transport time to a specialty center may be slightly longer than the time to an emergency department, but patients will receive definitive care more quickly.
4. Know the location of the centers in your area and the protocol for transporting a patient directly to one.
a. Sometimes air medical transport will be necessary.
b. Local, regional, and state protocols may guide your decision.
B. Interfacility transports
1. Many EMS agencies provide interfacility transportation for patients.
2. May include transferring patients to and from:
a. Clinics
b. Rehabilitation centers
c. Long-term care facilities
d. Hospitals
3. In certain rare circumstances, a nurse, physician, respiratory therapist, or medical team may accompany you with the patient.
#31 Lecture Outline
IX. Working With Other Professionals
A. Working with hospital staff
1. Become familiar with the receiving hospitals you will transport to.
Interact professionally with all hospital personnel who will be part of your patient’s care.
You may consult with appropriate medical staff by using the radio through established (online) medical control procedures.
#32 Lecture Outline
B. Working with public safety agencies
1. Some public safety personnel have EMS training and are better prepared than you to perform certain functions.
2. The best, most efficient patient care is achieved through cooperation among agencies.
#33 Lecture Outline
C. Community expectations
1. The community has expectations of EMS providers.
2. Whether you are in the public or private sector, encourage people in the community to become involved in your service to some level.
3. Focus on prevention.
4. You will work side by side with other professionals and groups.
5. It is vital that you understand your role and the roles of those with whom you interact.
#34 Lecture Outline
X. National EMS Group Involvement
A. National EMS group involvement overview
1. Many national and state organizations exist and invite paramedic membership.
a. Have an impact on the future direction of EMS
b. Provide access to valuable resources for developing:
c. Promote uniformity of EMS standards and practices
d. Some listed in Table 1-2
#35 Lecture Outline
XI. Professionalism
A. Professionalism overview
1. A profession is a field of endeavor that requires a specialized set of knowledge, skills, and expertise.
2. Attributes of a health care professional
3. As a paramedic, you will be measured by:
a. Standards, competencies, and continuing education requirements
b. Performance parameters
c. Code of ethics
#36 Lecture Outline
4. You are in a highly visible role in your community.
5. You must:
a. Instill confidence
b. Establish and maintain credibility
c. Continually show concern for the well-being of your patients and their families
#37 Lecture Outline
6. Your appearance is of utmost importance and has more impact than you may think.
a. Do not arrive at a call in dirty clothes, with dirty hands, or smelling offensively.
b. Appear and act like a professional at all times.
c. Professionalism holds no boundaries; saying you are only a volunteer or a part-time worker is not an excuse.
7. You must present a professional image and treat others in the profession with the respect with which you would want to be treated.
8. It is inappropriate to argue with other health care providers or hospital staff.
a. You are a patient advocate, but raise patient care issues professionally at appropriate times and locations.
b. Differences of opinion should be addressed by contacting a supervisor.
#38 Lecture Outline
9. Attributes of professionalism include:
a. Integrity
i. Openness, honesty, and truthfulness with your patients and coworkers
b. Empathy
i. Show your patients, their families, and other health care professionals that you identify and understand their feelings.
ii. It is okay to show emotions to some extent.
c. Self-motivation
i. Have an internal drive for excellence.
d. Confidence
i. Show you are confident in your skills and abilities.
e. Communications
i. Listen well.
ii. Speak directly, and do not use confusing medical terms.
f. Teamwork and respect
i. The paramedic is considered the team leader.
ii. Never undermine your team, but help guide and support the members.
g. Patient advocacy
i. Advocacy includes advocating for the patients you treat and for changes in the EMS system that will improve care or save lives.
ii. Always act in the best interests of the patient.
iii. Be on the lookout for spousal abuse, child abuse or neglect, and elder abuse or neglect.
iv. Report and communicate your findings to the appropriate authorities or as outlined in your state’s law.
h. Injury prevention
i. If you spot a potential hazard in the patient’s surroundings, diplomatically talk about it with the patient or a family member.
ii. Get involved with training programs such as those on the topics of fall prevention or child passenger safety.
iii. Discuss the use of bike helmets, safety belts, and child car seats whenever you can.
i. Careful delivery of service
i. Pay careful attention to details.
ii. Continuously evaluate and reevaluate your performance.
iii. Use other medical professionals as resources.
j. Time management
i. Prioritize your patient’s needs.
ii. Keep your emergency vehicle always ready to go.
iii. Document each emergency call as soon as it has concluded.
k. Administration
i. You may be asked to take on special projects or station duties.
ii. You may play a role in working with other agencies and forging partnerships with other public safety resources.
iii. You may be appointed to a leadership position within your organization; this is your opportunity to help others achieve their goals within your service.
10. More health care locations are using paramedic services within their organizations.
a. Hospital emergency departments and clinics
b. Physician offices
c. Local public health departments
d. Home health organizations
#39 Lecture Outline
XII. Roles and Responsibilities
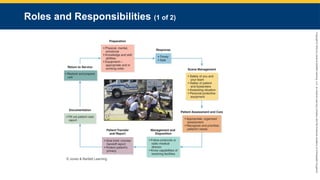
A. Some of the paramedic’s primary responsibilities (shown in Figure 1-11) include:
1. Preparation
a. Be prepared physically, mentally, and emotionally.
b. Keep up your knowledge and skill abilities.
c. Have the appropriate equipment for your call.
2. Response
a. Responding to an event in a timely, safe manner.
b. Never run “hot” without regard for the safety of yourself, your partner, your patient, and other people on the highway.
3. Scene management
a. Ensuring your own safety and the team’s safety is the first priority.
b. You must also ensure the patient’s safety and the safety of any bystanders.
c. Prior to reaching the scene, consider all possibilities from the dispatch information.
d. Use of personal protective equipment (PPE)
4. Patient assessment and care
a. Perform an organized assessment of all patients.
b. Recognize and prioritize the patient’s needs.
5. Management and disposition
a. Follow approved guidelines or protocols.
b. Contact medical control if needed.
c. Know the capabilities of the receiving facility.
6. Patient transfer and report
a. Once you arrive at the receiving facility:
i. Give the appropriate facility staff a brief, concise handoff report.
ii. Use discretion to protect your patient’s privacy.
7. Documentation
a. It is extremely important that a patient care report be filled out ASAP.
b. If a report is not possible or required, inform the facility how to reach you if providers there have a question.
c. The report serves as a legal record of all aspects of the call.
8. Return to service
a. Restock and prepare the unit as quickly as possible.
#40 Lecture Outline
B. Never miss an opportunity to teach the community about injury and illness prevention.
1. Explain to people how to appropriately use your services.
2. In areas where trained EMS staff is limited, promote programs that get the public involved in CPR or automated external defibrillator (AED) training.
3. In some regions, paramedics may be responsible for working in clinics, freestanding emergency facilities, and hospitals.
4. For influenza and possible pandemic issues, paramedics and home health nurses are now being asked to:
a. Provide some immunization and medication administration
5. Set out a well-thought campaign for EMS.
a. Research your community.
b. Look at strengths and weaknesses of the system.
c. Develop initiatives to improve the system.
6. Involve yourself in your community to educate the media and public and advocate for EMS.
#41 Lecture Outline
XIII. Medical Direction
A. Paramedics carry out advanced cardiologic, pharmacologic, and trauma care skills.
1. They cannot act independently.
2. They must take direction from a medical director.
B. EMS medical directors may:
1. Educate and train personnel
2. Recommend or select new personnel and equipment
3. Develop clinical protocols or guidelines with other EMS experts
4. Develop and assist in a quality improvement program
#42 Lecture Outline
5. Provide input into patient care
6. Interface between EMS systems and other health care agencies
7. Serve as an EMS advocate to the community
8. Serve as the medical conscience of the EMS system
#43 Lecture Outline
9. Provide online and off-line medical control
a. Online (direct) medical control: Given in real time by radio or other electronic communication
b. Off-line (indirect) medical control: given through a set of protocols, policies, and/or standards developed by or with the approval of your medical director
c. Online medical control:
i. Provides immediate and specific patient care resources
ii. Allows telemetry transmission (in some locations, video telemetry is available)
iii. Allows for continuous quality improvement
iv. Can offer on-scene assistance
d. Offline medical control allows for the development of:
i. Protocols or guidelines
ii. Standing orders
iii. Procedures
iv. Training
10. Perform or help with patient care report reviews
#44 Lecture Outline
XIV. Improving System Quality
A. One way to improve quality is through continuous quality improvement (CQI).
1. Tool used to continually evaluate your care
2. Quality control: Another process that evaluates problems and finds solutions
3. CQI is a process of assessing current practices and looking for ways to improve
4. A dynamic process
5. A good CQI process should the following steps:
a. Identify any departmental or system-wide issues
b. Identify specific items that need to be measured
c. Conduct an in-depth review of the issue(s)
d. Evaluate the issue(s) and develop a list of remedies
e. Develop an action plan for correction of issue(s)
f. Enforce a plan of action and include time frames
g. Reexamine the issue
h. Identify and promote excellence found in patient care during the evaluation
i. Identify modifications that may be needed to protocols and standing orders
j. Identify situations that are currently not addressed by protocols or standing orders
#45 Lecture Outline
B. A CQI program can help to prevent problems by evaluating day-to-day operations and identifying possible stress points, including:
1. Medical direction issues
2. Education
3. Communications
4. Prehospital treatment
5. Transportation issues
6. Financial issues
7. Receiving facility review
8. Dispatch
9. Public information and education
10. Disaster planning
11. Mutual aid
#46 Lecture Outline
C. Whenever possible, all emergency calls should be reviewed.
1. Ultimately, the focus of CQI needs to be on improving patient care.
2. Use your CQI process as a constructive tool for continuous improvement.
D. CQI can be in the form of a peer review.
1. CQI can be a good learning experience if proper and consistent guidelines exist and those reviewing keep an open mind.
2. Everyone makes mistakes and misses things from time to time.
a. Peer recommendations for improvement should be educational tools.
3. In an ideal system, members of the peer review team rotate.
#47 Lecture Outline
E. Look for ways to eliminate human error.
1. Ensure adequate lighting when handling medications.
2. Limit interruptions.
3. Keep medications in a specific location and in their original packaging.
4. Handing patients off is a high-risk activity.
5. It is important that you understand the circumstances that cause errors to help you identify those that can be prevented.
6. There are three primary sources of errors:
a. Rules-based failure (example: legal right to administer medication)
b. Knowledge-based failure (example: knowing all pertinent information about a medication)
c. Skills-based failure (example: proper use of equipment)
#48 Lecture Outline
7. Agencies need clear protocols.
8. Be aware of your environment.
a. Limit distractions.
b. Ensure you can find what you need in a timely manner.
9. When performing a skill, ask yourself, “Why am I doing this?”
10. Use cheat sheets.
11. Be conscientious of protocols, and do not allow interruptions when providing care.
#49 Lecture Outline
XV. EMS Research
A. EMS and evidence-based practice
1. Protocols should be based on scientific findings.
2. The Department of Transportation National EMS Research Agenda has described processes and set goals to optimize prehospital care.
3. A publication at the ems.gov website titled Progress on Evidence-Based Guidelines for Prehospital Emergency Care outlines some of the progress in relation to research findings.
4. Historically, EMS operations have been standardized and not evidence based.
B. Education of researchers
1. Research is typically performed by properly educated researchers, those with a PhD or MD degree, but anyone can be part of research if properly trained.
C. EMS college track for paramedics
1. There has been an increase in the number of accredited colleges and universities that provide an EMS track for paramedics.
2. Graduates can enter the field as a trained paramedic with a bachelor’s degree.
3. These institutes also produce high-quality research.
4. Paramedic students may have the opportunity to assist in a research project that will eventually change the future of EMS.
#50 Lecture Outline
D. The research process
1. Identify the specific problem, procedure, or question to be investigated.
2. Carefully reviewing the research—in its entirety—is very important.
a. Some research topics are driven by a product manufacturer or an entity that is strictly out to prove something right or wrong regardless of its importance in EMS.
3. Once the question is determined, develop a research agenda by specifying:
a. Questions to be answered
b. Specific aims to be addressed
c. Methods by which the study will be carried out
d. Methods to gather data
4. Additional questions may result from the study, but the researcher must stick to the research agenda and answer the specific questions at hand.
a. Other questions may become topics in a separate study.
#51 Lecture Outline
5. Once a question has been decided, the researcher must determine the research domain (area of research).
a. Research domain: The area of research
b. Domains include:
i. Clinical
ii. Basic science
iii. Systems or operations
iv. Education on how programs are taught
6. A research consortium is a group of agencies working together to study a topic.
a. Paramedics may be involved in collaborative research by gathering data.
i. You may be asked to:
(a) Identify certain populations for research
(b) Gather volunteers from calls you are on
ii. If you are asked to identify patients, have some information with you regarding the research.
(a) If a patient agrees to become part of the research, obtain informed consent from the patient specifically for the research and note this in your patient care report.
iii. It is crucial that initiatives associated with research never take priority over care the patient may need.
#52 Lecture Outline
E. Funding
1. Researchers should use an institutional review board (IRB) before a project begins.
a. Approval of an IRB is required to ensure that the rights of study subjects are protected throughout the study.
b. An IRB is a group or institution that reviews research.
2. Major research requires specific funding.
3. Funding can come from:
a. Local or federal government
b. Nonprofit foundation grants
c. Industry or corporate funding
4. Studies must go through an evaluation process to ensure they will answer a question in the domain covered by the grant.
a. The methods and results are subject to stipulations placed on them by the grantor.
b. Before applying for a grant, ensure you meet all the criteria and can adhere to the expectations throughout the entire project.
5. Any type of support given to a researcher is considered funding.
a. Free lab space
b. Travel
c. Assistants to help with the research
6. To prevent bias or conflicts of interest, researchers should:
a. Disclose all sources of funding and support
b. Maintain total transparency regarding research methods
#53 Lecture Outline
F. Types of research
1. Depends on the topic and what the researcher wants to learn
2. Qualitative research
a. Focuses on questions within surrounding events and concurrent processes
b. Attempts to build a more complete, holistic picture
c. Takes into account real-world factors that may have influenced the study
d. Often used when answers cannot be identified in quantitative research
i. Usually involves the researcher’s interpretation of previously published data and yields a statement of the findings
e. Investigates the why and how of decision making
i. Not just what, where, and when
f. No set guidelines
i. Each study must have parameters specific to the question.
g. Sometimes medical research
3. Quantitative research
a. Based on numeric data
b. Three types:
i. Experimental research
(a) Scientific approach
(b) Researcher controls, manipulates, and measures variables to determine how manipulating the variables affects subjects.
(c) Concerned with cause-and-effect relationships
ii. Nonexperimental research
(a) Descriptive research
(b) Does not use patients and manipulating variables
(c) Example: for pain management studies, data would be gathered through interviewing and watching vital signs
iii. Survey research
(a) Conclusions are based on survey results.
(b) Researchers must identify what is being measured and determine the appropriate sample size.
(c) Sample populations must reflect the composition of the population being researched.
#54 Lecture Outline
4. Retrospective research
a. This type of research uses available data (medical records or patient care reports).
i. Example: Examine available data to determine the types of calls that occur at night versus daytime or the number of calls where substance abuse was the cause of the patient’s complaint
b. Retrospective research may be used to:
i. Develop educational sessions for EMS personnel
ii. Plan public education and public prevention strategies
c. Researchers may need to collaborate with a hospital or group of hospitals in gathering data.
d. In large studies, data is often collected from widespread patient databases.
e. Techniques used by large studies to gather and analyze data can be used at the local level.
#55 Lecture Outline
5. Prospective research
a. Gathers information as events occur in real time
6. Cohort research
a. Examines patterns of change, a sequence of events, or trends over time within a certain population
7. Case study
a. Investigation and documentation of a single case over a specific period
8. Cross-sectional design
a. “Snapshot” of all data at one point in time
9. Longitudinal design
a. This design collects information at various set time intervals.
b. Prospective studies must have a longitudinal data-gathering method.
c. Retrospective, cohort, or case study research can use either a cross-sectional or longitudinal data collection technique.
10. Literature review
a. Analyzes existing literature to draw a conclusion
#56 Lecture Outline
G. Research methods
1. The first step in research is to identify the group(s) necessary for the research.
2. Once eligible subjects are identified, researchers randomly choose who will be involved in the research.
3. There are many ways to select subjects to be part of the research.
a. Systematic sampling: When a list of research subjects or groups is computer generated
b. Alternative time sampling: Time frame parameters can be set.
c. Convenience sampling
i. Manually assigned to a specific researcher
ii. Not random
iii. Least preferred method
4. Even in the best cases, sampling errors can occur.
a. A study may fail to include all of the needed subjects.
b. The study may have included people who meet criteria but still are not the best representation.
It is recommended you select a much higher number than you need so you allow for those who will not complete the study or will fall out of the research parameters.
6. Determine the appropriate population size.
a. Use a power analysis to avoid type II error (not finding the difference between two or more groups when one exists).
b. Determine the variance (variability of findings in the target population).
c. Conduct a pilot study.
7. Parameters should be identified.
a. Outline the type of people who are appropriate for the study.
#57 Lecture Outline
8. Studies can be blinded or unblinded.
a. Blinded: Investigators are unaware of the study arm into which the subject being interviewed has been enrolled.
b. Unblinded: Participants are advised of all aspects of the project.
9. Gathered research statistics can be in a descriptive or inferential format.
a. Descriptive: Observations are made, but no attempts are made to alter or change an event.
b. Inferential: A hypothesis is used to prove one finding over another.
c. Descriptive statistics can be performed in a qualitative or quantitative style.
10. Standard deviation outlines how much the values in a set of data differ from the mean.
#58 Lecture Outline
H. Ethical considerations
1. The organization’s IRB monitors whether a study is conducted ethically.
a. Ensures the protection of study participants
b. Ensures appropriate conduct
2. Any risks to study subjects must not outweigh potential benefits.
3. Potential conflicts of interest must be identified.
#59 Lecture Outline
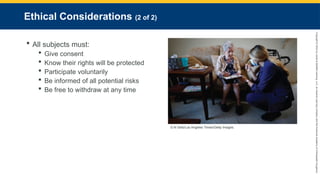
4. All subjects must give consent and be certain their rights and welfare will be protected.
5. Subjects must participate voluntarily.
6. Subjects must be informed of all potential risks involved and be free to withdraw.
7. At minimum, subjects should be advised they are protected by the Office of Human Research Protections.
8. To ensure accurate research, the potential for subject withdrawal or other variables that may affect the outcome should be identified before the study begins.
9. Potential participants in a clinical domain research trial must be informed about the study protocols prior to participating.
#60 Lecture Outline
I. Evaluating medical research
1. When evaluating an article, look for certain criteria to determine the research quality.
a. Refer to Table 1-3 for the questions you should answer.
2. Once you have identified the type of study, its methods, and its strengths, look at the body of the study itself.
3. To start, determine what the hypothesis of the study is, and whether the population base matches your region.
a. Valid studies have:
i. A clearly stated hypothesis
ii. Clearly defined outcome measurements
b. Avoid studies with vague hypotheses or outcome measurements.
c. The more subjects involved in a study, the more relevant the data is likely to be.
4. Look at the patient and selection criteria.
a. For a study to be valid, all subjects need to be accounted for, even if they did not make it into the final outcome.
5. Determine how the data was analyzed.
a. Ensure the methods of analysis are appropriate for what the study is designed to measure.
6. Identify the authors of the study and their conclusions.
a. Be certain their conclusions are not biased based on financial or other conflicts of interest.
7. Determine whether the outcome and results are significant, both statistically and clinically.
a. Statistical significance: Describes how often the results of a study may happen by chance.
b. Clinical significance: Is the finding effective in enough patients to make it a useful treatment for the majority?
8. Consider the type of journal in which the research is published when determining quality and validity.
#61 Lecture Outline
9. One method for ensuring quality is through peer review.
a. Peer review: Studies are sent to other subject matter experts for review of the content and research methods prior to publication.
b. The research and its conclusions are accepted, revised, or rejected based on the findings of the peer review.
10. Internet sites can be useful tools for accessing research, including:
a. Google Scholar
b. Medscape
c. PubMed
11. Research studies must follow a structured process.
12. There will always be limitations to what can be measured and how accurate measurements can be.
#62 Lecture Outline
J. Evidence-based practice
1. Patient care should be focused on the procedures that have proven useful in improving patient outcomes.
2. EMS providers should stay up-to-date on the latest advances in health care.
3. To ensure quality evidence, researchers often rate the quality of a study.
a. There are many different rating systems.
i. Example: The American Heart Association assigns class (strength) of recommendation and levels (quality) of evidence.
#63 Lecture Outline
4. Research determines the effectiveness of treatment.
a. EMS must prove what it does makes a difference to help secure funding.
5. Research can help identify which procedures, medications, and treatments work and which do not.
6. When following a new study’s recommendations, your service should measure the results in your CQI program.







































































![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)
















