#2 Lecture Outline
I. Introduction
A. Clear communications: a core emergency EMS skill
1. You must be able to communicate with:
a. The dispatch center
b. Other members of the EMS system
c. Patients, family members, and bystanders
2. Factors that influence how effectively you communicate include:
a. Communication style
b. Knowledge level
c. Ability to listen and comprehend
d. Ability to accurately convey information
e. Life experience
3. Communication can be affected by your tone of voice, body language, and ability to use technology.
#3 Lecture Outline
B. Communication theory
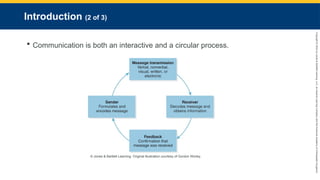
1. Communication is both an interactive and a circular process.
2. The sender formulates and encodes the message to be sent.
a. Encoding involves determining the words or ideas to be sent and formatting the information for transmission.
3. The message is transmitted to a receiver.
4. The receiver receives and decodes the message to get the information being relayed.
5. The most common methods of transmitting information include:
a. Verbal
b. Nonverbal
c. Written
d. Visual
e. Electronic
6. The final step in effective communication is feedback.
a. Confirmation by the receiver that the message was accurately received
b. Permits clarification if a message was unclear
#4 Lecture Outline
C. Barriers to effective communication
1. Potential barriers to communication include:
a. Language barriers
b. Vision or hearing impairment
c. Impaired cognition or confusion
d. Psychiatric conditions
e. Substance abuse
f. Preexisting medical conditions
g. Lack of ability to comprehend
h. Stress
i. Preconceptions
2. Adjust how you communicate to minimize barriers.
3. Your attitude and demeanor can also affect communication.
4. Treat every patient you encounter professionally.
#5 Lecture Outline
II Response to the Call for Emergency Medical Services
A. Crew resource management
1. An operational practice developed by the US Air Force and the airline industry
2. Designed to enhance communication and teamwork and reduce preventable errors
3. Involves all members in flight safety; encourages members to:
a. Pay attention
b. Voice concerns
c. Participate in the decision-making process
4. Use a sterile cockpit concept:
a. All attention is placed on the safety of the crew and surroundings during takeoff and landings.
b. EMS should use this concept when responding to calls and during patient transport.
#6 Lecture Outline
5. In practice, CRM:
a. Begins with a prebriefing while en route to the call
b. On scene, there are frequent check-ins and updates, reassessments of the situation, and fine-tuning of the plan as necessary.
c. Crew members should cross-check each other when a high risk of errors exists.
i. Example: Double-checking medication doses when treating a pediatric patient
d. Every team member is responsible for situational awareness and letting others know of problems or risky situations.
6. CRM training and practice should be part of EMS education.
#7 Lecture Outline
B. Phases of EMS dispatch
1. All EMS calls originate when someone recognizes that a potential medical emergency exists and reports it to the local emergency response system.
a. In the United States, this is accomplished by calling 9-1-1.
2. The call is automatically routed to a public safety answering point (PSAP).
a. Primary PSAP may either dispatch resources directly or route the call to a secondary PSAP, such as a specialized EMS dispatch center.
C. Information gathering
1. When a 9-1-1 call comes in, the dispatcher will try to elicit the following information:
a. Exact location of the patient(s)
b. Telephone number of the caller
c. Why EMS was called
d. Information about the patient’s condition
e. Details about the location
f. Information about the situation
D. Dispatch
1. As soon as the dispatcher has obtained the address of the emergency, the telephone number of the caller, and the nature of the emergency, the dispatcher will determine which resources need to be dispatched and notify these resources.
2. After the ambulance is dispatched, the dispatcher will return to the caller to obtain the rest of the information and relay this information while the responding unit is en route.
3. This process permits:
a. The EMS crew to determine whether to respond using the lights and siren (based on local protocols) and
b. To anticipate and prepare for any tasks that may need to be performed at the scene
#8 Lecture Outline
E. Computer-assisted dispatch
1. Most EMS systems utilize computer-assisted dispatch (CAD) systems.
2. Enables the dispatcher to view all information about the call, including:
a. Information received from the caller
b. Times of events
c. Visual prompts that list key questions to ask the caller
3. It may also display additional information provided by the enhanced 9-1-1 system, such as:
a. Maps
b. Fastest route to the call location
c. Prior calls to the same address
d. Known hazards at the call location (eg, toxic chemicals stored, dangerous pets)
4. The CAD system may make recommendations about which EMS units to dispatch based on location and response times.
5. The dispatcher can send all of this information to the EMS crew via the mobile data terminal (MDT), with the crew able to see information displayed on the CAD terminal.
#9 Lecture Outline
F. Advice to the caller
1. After dispatching the appropriate resources and alerting responders to any special circumstances, the dispatcher will return to the telephone and inform the caller what is happening.
a. The dispatcher may be able to provide prearrival medical instructions to the caller through the EMD program.
#10 Lecture Outline
G. Ongoing communications with responding units in the field
1. The dispatcher must always remain aware of what is occurring in the field and stay in contact with the ambulance and other responders.
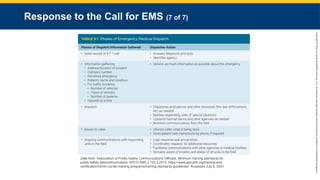
2. The phases of the emergency medical dispatch process and the dispatcher’s roles are summarized in the table.
#11 This table shows the phases of emergency medical dispatch.
#12 Lecture Outline
III. EMS Communications Systems
A. A variety of communications equipment
1. Communication systems and devices use radio signals to send and receive information (basic two-way radio, computerized radio systems, cellular technology).
2. Backup communication systems are essential.
#13 Lecture Outline
B. Basic radio communications theory
1. A radio transmits signals by electromagnetic waves.
2. The basic radio wave in which a signal is encoded is called a carrier wave.
C. Radio frequencies
1. The radio frequency is the number of oscillations (or cycles) per second of the carrier wave (measured in hertz).
2. Common abbreviations are:
a. Hertz (Hz)—cycles per second
b. Megahertz (MHz)—1 million cycles per second
c. Gigahertz (GHz)—1 billion cycles per second
3. Frequencies are grouped into bands by the Federal Communications Commission (FCC) for specific purposes.
a. Two most commonly used bands for medical communication are the very high frequency (VHF) band and the ultrahigh frequency (UHF) band.
i. The VHF band extends from 30 to 300 MHz.
ii. The UHF band extends from 300 MHz to 3.0 GHz.
D. FCC narrow-band standards
a. Since January 1, 2013, frequencies in the public safety radio spectrum between 150 to 174 MHz and 421 to 470 MHz have been reassigned with a spacing of 12.5 KHz, referred to as narrow-band technology.
i. Radios using the older 25 kHz technology are obsolete.
ii. This system has doubled the number of frequencies available for public safety and EMS use and supports newer, more sophisticated digital radio systems.
#14 Lecture Outline
E. Radio signals
1. Radio communications require two types of devices.
a. A transmitter takes data or sound, converts it into a radio signal, and transmits it on the designated frequency.
b. A receiver collects the radio signal and translates it back into data or sound.
c. Transceivers (two-way radios) contain both a transmitter and a receiver.
d. Range is a limiting factor affecting all radio signals.
i. Depends on output power, frequency being used, location and size of the antenna, and whether or not an uninterrupted path to the receiver exists
e. Background noise is present on all radio frequencies.
i. Radio receivers are equipped with a filtering system known as squelch.
#15 Lecture Outline
F. Communication system components
1. Base stations
a. Transmitter output power of up to 275 W
b. Have a fixed location (dispatch center or hospital)
c. Serve as dispatch and coordination areas
d. Have a large antenna
i. Usually situated on top of a building or a tall mast
e. Often capable of operating on multiple frequencies and bands
2. Mobile transceivers
a. Two-way radios mounted on vehicles and aircraft
b. Antenna externally mounted on the vehicle
c. Output power from 5 to 50 W
d. Line-of-sight range can extend up to 15 miles
#16 Lecture Outline
3. Portable transceivers
a. Small battery-powered units
b. Also known as “handhelds” or “walkie-talkies”
c. Range is usually limited to 3 to 5 miles
d. Useful when you must work at a distance from your vehicle
4. Radio systems
a. Simplex
i. All transmissions on the same frequency
ii. Allow multiple users to communicate with each other using one common frequency
iii. Usually used only for short-range communications
b. Duplex
i. Radio signals are transmitted on one frequency and received on a second frequency.
ii. Semi-duplex systems allow communication in only one direction at a time; full-duplex systems allow continuous communication in both directions at the same time.
c. Multiplex
i. Utilize radio signals to carry multiple streams of audio and/or data at the same time
ii. Used to transmit voice and ECG tracings (biotelemetry)
d. Digital
i. Allow the transmission of digital signals (computer) or analog (voice) signals that have been digitized and compressed by a computer
ii. Can communicate with other digital and analog radios
#17 Lecture Outline
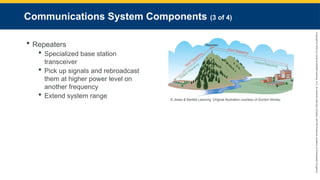
5. Repeaters
a. A specialized base station transceiver with a powerful transmitter and a large antenna
b. Typically located on a high spot such as a tower, mountaintop, or tall building
c. Pick up signals and rebroadcasts them at higher power level on another frequency
i. Extends the range of low-power portable radios
ii. Allow the radio system to cover a larger geographic area and bypass obstacles
#18 Lecture Outline
d. Sharing of frequencies and repeaters via encoded radio signals
i. Allows multiple users to share frequencies and repeaters.
ii. Continuous Tone-Coded Squelch System (CTCSS) is the most common type in public safety.
iii. Those who have a CTCSS decoder will be able to receive the transmission; receivers without it will not.
iv. Dual-Tone Multi-Frequency (DTMF) system tones are encoded using a keypad on a transmitter.
v. DTMF is used most frequently by systems using UHF-band Med channels.
6. Digital trunked radio systems
a. Sophisticated digital communications network operating in the 800 and 900 MHz UHF bands.
b. These systems utilize multiple repeaters and computers to route radio traffic within the system.
c. The transceiver is set to a channel or mode rather than a frequency.
d. Each mode is designated for a particular purpose.
e. The network assigns each transmission to the next available frequency.
7. Radio dead spots
a. Dead spots are areas where mobile or portable radios are unable to communicate with a repeater or each other.
b. Dead spots may be caused by distance or obstructions.
c. You must learn the locations of radio dead spots in your service area.
d. You may need to use alternative communication systems or establish a temporary relay station.
#19 Lecture Outline
G. Interoperability
1. Local agencies enter into mutual aid agreements with neighboring or regional jurisdictions to offer assistance to one another in the event of a large-scale incident.
2. Each agency’s communications system must be compatible with that of the other agency.
a. This principle is referred to as interoperability.
3. The US Department of Homeland Security developed the SAFECOM communications program to address the issue of incompatible radio systems between agencies.
a. These national interoperability standards, released in 2006, are intended to develop “a system of interoperable public safety communications across all local, tribal, state, and federal ‘first responder’ communications systems.” (US Department of Homeland Security)
b. These standards:
i. Identify the use of nationally standardized frequencies for disasters and other communications
ii. Are used for interstate and national events
(a) Each state has established its own internal standards for interoperability between local jurisdictions, which are to be used for MCIs and other local mutual aid responses.
4. The Project 25 (P25) standards are digital radio hardware standards established by the Association of Public-Safety Communications Officials.
a. Ensure the pieces of digital radio equipment supplied by different manufacturers to public safety communications community are compatible with one another.
#20 Lecture Outline
H. Cellular technology
1. Cell phones are commonly used in EMS communications systems.
a. Low-power portable radios
b. Communicate through interconnected repeater stations called cells
c. Linked by computer systems
d. Connected to the telephone network
2. Paramedics need to know:
a. Commonly used phone numbers
#21 Lecture Outline
3. Telephone calls may be patched into radio networks, enable direct communication between a paramedic using a radio in the field and another party using a telephone, such as medical control
a. The phone patch allows for recording.
i. Important when requesting orders or permission to perform a procedure
4. Smartphones have brought previously unheard-of capabilities to the EMS provider. They allow users to:
a. Communicate wirelessly using voice, text, and video
b. Take and send photographs or videos to other devices
c. Use GPS receivers with mapping software
d. Access a huge range of medical applications
e. You must be aware of the privacy implications of taking photographs or videos using smartphones or tablets.
#22 Lecture Outline
5. Automatic crash notification (ACN) technology is another evolving use of cellular technology.
a. Utilize specialized onboard computers in motor vehicles to send data to a monitoring station in the event of a crash, including:
i. Geographic location of the crash
ii. Vehicle type
iii. Severity of the crash
iv. Principal direction of force at the point of impact
v. Whether seat belts were in use
vi. Whether airbags were deployed
b. May allow direct two-way voice communication with the occupants of the vehicle
#23 Lecture Outline
I. Satellite communications
1. Satellite telephones can be valuable in rural and remote areas with unreliable or absent radio and cell phone coverage.
2. The global positioning system (GPS) is a satellite network that utilizes handheld or vehicle-mounted receivers to locate the user’s position and provide directions to other locations.
a. Geographic information system (GIS) technology utilizes computerized GPS mapping systems to:
i. Track and predict ambulance response times
ii. Determine the distance to the closest trauma center or other hospitals from specific locations
iii. Track the frequency of motor vehicle crashes and the severity of injuries from different geographic locations
iv. Determine the location of emergency helipads
v. Provide other information useful in EMS systems operations and planning
3. Satellite distress beacons and messengers can be a worthwhile safety technology for ambulances and emergency medical personnel who operate in rural or remote locations, or during search and rescue or disaster operations.
#24 Lecture Outline
J. Backup communications systems
1. All EMS and public safety communications systems need to have some type of backup.
2. The most commonly used backup system is an alternative radio system, typically one that relies on basic technology such as VHF or UHF simplex and duplex radios and redundant repeaters.
3. Almost every EMS system uses landline and cell phone networks as a backup to other communication technologies.
4. Backup systems should also include generators at dispatch centers and hospitals.
5. In disaster situations, having redundant or backup systems is essential.
a. Backup plan may include the use of amateur radio groups.
i. Amateur Radio Emergency Service (ARES)
ii. Radio Amateur Civil Emergency Service (RACES)
#25 Lecture Outline
K. Biotelemetry
1. Biotelemetry is the measurement and transmission of vital signs and other physiologic data to a remote terminal.
2. It is mostly used to send ECG data to the medical control physician or ED.
3. ECG telemetry has been used less frequently because EMS systems now rely on paramedics to assess cardiac rhythms and make independent treatment decisions.
4. Advances in medicine and communications technology occurred to make ECG telemetry a valuable EMS tool.
a. The national standard of care for patients with an acute ST-segment elevation myocardial infarction (STEMI) is percutaneous coronary intervention (PCI).
i. Rapid transport of patients to the closest primary PCI hospital/STEMI receiving center and short “door-to-balloon” times have resulted in much better patient outcomes.
b. Cell phone, broadband networks, and digital radio systems made it possible to transmit a 12-lead ECG from the field to a hospital.
5. Telemedicine technology uses specialized computer terminals and networks that permit secure two-way transmission of diagnostic data.
a. Allows the interactive exchange of information between the paramedic and the medical control physician
b. Can facilitate rapid assessment and treatment of a wide range of conditions and patients in the prehospital setting
6. Advancements in technology are occurring rapidly.
a. EMS systems must keep up with the technology that can improve communication of patient information.
#26 Lecture Outline
IV. Communicating by Radio
A. The effectiveness of the EMS communication network depends on:
1. Technical hardware/software
2. People who use it
#27 Lecture Outline
B. FCC regulations
1. The FCC is the agency that regulates US radio and television communication.
2. The FCC:
a. Issues radio licenses
b. Allocates frequencies
c. Develops technical standards
d. Establishes and enforces rules and regulations for operating radio equipment
3. The FCC monitors transmissions on various frequencies and conducts spot checks of base stations to ensure they are licensed.
4. Fines and other penalties can be imposed for failing to follow FCC rules and regulations.
#28 Lecture Outline
5. The FCC requires that frequencies allocated for public safety and EMS communications are confined to that use.
a. Use of obscenities and transmissions unrelated to the provision of EMS are forbidden.
6. To communicate a personal message, the dispatcher should call recipient’s personal cell phone or notify recipient by radio to contact the base by phone.
#29 Lecture Outline
C. Clarity of transmission
1. The following guidelines can improve the clarity of your transmissions:
a. Know what you want to say before beginning your transmission.
b. Before you begin to transmit, make sure the radio is turned on, check the volume, and then listen to make sure the channel is clear.
i. If another radio transmission is in progress, wait until the parties have finished transmitting before you try to transmit.
c. Keep your mouth close to the microphone, but not too close.
i. About 2 to 3 inches is usually ideal.
d. After the channel is clear, press the push-to-talk (PTT) key for at least 1 second before you start speaking.
i. Ensures that the beginning of your message is not lost
e. Start your transmission with the identifying information.
i. The number or the name of the unit being called first
ii. Then your own identification
f. Wait for a response to ensure the other station is listening.
g. Speak slowly and clearly, pronouncing each word carefully.
h. Do not shout.
i. Keep calm, and keep your voice free from emotion.
j. Use plain language and only use radio codes that are specifically approved by your system and that everyone will understand.
k. If you have a lot of information to convey, then break your transmission into short (30-second) chunks.
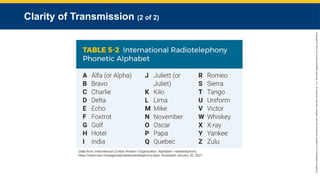
l. When speaking a word or name that might be misunderstood, spell it out, using the International Radiotelephony Phonetic Alphabet or a similar system.
m. When presenting numbers that might be misunderstood, transmit the number as a whole, then digit by digit.
n. Confirm receipt of all replies.
o. Indicate when your transmission is completed.
#30 This table shows the international radiotelephony phonetic alphabet.
#31 Lecture Outline
D. Content of transmissions
1. Radio transmissions should be accurate and concise.
2. Guidelines for what you should and should not include in EMS radio communications include:
a. Remember, anyone may be listening.
b. Protect the privacy of the patient at all times.
i. Do not use patient’s name on the air.
ii. Do not transmit personal information about the patient.
iii. Follow HIPAA guidelines and local laws.
iv. Do not say anything on the radio or phone you would not want others to hear.
c. Be impersonal.
i. Use “we,” not “I,” to refer to yourself.
ii. Use proper names and titles to refer to others when necessary.
d. Use proper and correct medical terminology.
e. Avoid using words that are difficult to hear.
i. Examples: “Affirmative” instead of “yes,” “negative” instead of “no”
f. Act professionally.
g. When you receive instructions by radio from dispatch or from medical control, echo the order back to make certain you have understood it correctly.
h. Question any orders you did not hear clearly or did not understand.
i. If you have a lot of information to convey, then break your transmission into short (30-second) chunks.
j. When you finish transmitting, notify the receiver that the transmission is finished.
#32 Lecture Outline
E. Codes
1. The 10-code system and other radio codes have been phased out in most EMS systems.
2. A medical priority dispatch system (MPDS) is used by many EMS systems.
a. It uses a specific format to indicate the nature of the emergency and the priority.
b. The dispatcher uses this information to decide the priority and response mode when assigning the responding units.
3. The National Incident Management System (NIMS) discourages the use of all radio codes.
a. The preferred format is clear text.
F. Clear text communications
1. The preferred communications format in many systems
2. Simply means using everyday language and accepted terms to communicate
#33 Lecture Outline
V. Communications Formats Used During the Different Phases of the Response
A. Different formats for each agency’s or region’s radio and other communications
1. Familiarize yourself with the format(s) used in your area.
B. Dispatch communications
1. Respond to the dispatcher that you have received the message.
a. Confirm the location and call reference.
i. Ensures there has been an effective and accurate transfer of information
ii. Establishes your dispatch time
#34 Lecture Outline
C. Response to the scene communications
1. As you travel toward the scene, notify dispatch.
a. Lets them know you are on the way and establishes your en-route time
2. Your next transmission should be at your arrival on scene.
a. Allows you to update dispatch and establishes your arrival time
b. Any time you determine that additional resources are needed, request them.
#35 Lecture Outline
D. On-scene and tactical communications
1. You need to stay in contact with other responders at the scene.
a. This is typically accomplished using a portable radio on an assigned tactical channel.
b. Large-scale incidents may need a more involved communication plan.
E. Patient transport communications
1. After you have treated your patient(s) and are ready to provide transport, inform dispatch.
a. Establishes a time stamp for departing the scene
b. Documents the fact that you have completed operations at the scene, are on the way to the hospital, and the response is nonemergent
2. The next radio transmission to dispatch is to notify them of your arrival at the medical facility.
a. Confirms arrival at the hospital
b. Establishes status of your unit
c. Documents the unit’s unavailability for further service at this time
3. Once you have turned over patient care, given your report, and restocked the ambulance, update dispatch that you are back in service.
#36 Lecture Outline
VI. Relaying Information to Medical Control
A. Legal basis for paramedic practice
1. Off-line medical control allows a paramedic to perform certain procedures or treatments based on protocols or standing orders without physician contact.
2. Online medical control is when the physician gives patient-specific orders and instructions directly to the paramedic by radio or telephone.
3. Radio communications between paramedics and physician should be clear, concise, and accurate.
4. Using a standard format for communicating patient information ensures that it is relayed consistently and completely.
#37 Lecture Outline
B. Format for reporting medical information
1. The keys to a good radio report are:
a. Be organized.
b. Know what you want to say before beginning your transmission.
c. Include all required information.
2. The following medical information should be included in a report:
a. Destination facility and estimated time of arrival (ETA)
b. Patient’s age and sex
c. Patient’s chief complaint
d. Brief, pertinent history of present illness or injury
e. Medications and important allergies
f. Anything else from patient’s medical history relative to current situation, including major underlying medical conditions
g. Patient’s level of consciousness and degree of distress
#38 Lecture Outline
h. Patient’s mental status
i. Patient’s vital signs
j. Pertinent physical findings in head-to-toe order
k. ECG findings
l. Treatment given so far and response to treatment
#39 Lecture Outline
3. Transmit information quickly, completely, and in a well-organized fashion.
4. Continue to monitor and assess the patient; report any changes.
#40 Lecture Outline
C. In-person report and transfer of care communications
1. The final phase of your patient care communication is your bedside report to the receiving facility medical and nursing staff.
2. Relay all pertinent information. Use the same format as your radio report and share any information that was not already provided.
3. Keep in mind the patient and family may be listening.
4. Answer all questions from the medical and nursing staff.
5. Patient handoff also involves written documentation.
#41 Lecture Outline
D. Medical terminology
1. Learn established medical terms and abbreviations.
a. Your EMS system may have approved lists of terms.
#42 Lecture Outline
VII. Therapeutic Communication
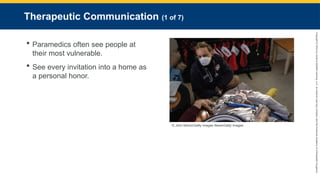
A. People at their worst and most vulnerable
1. At least one-half of calls involve entering people’s homes at all hours at very private moments.
2. Treat each invitation into a home as a personal honor in a time and place where few would be welcome.
#43 Lecture Outline
3. You will often work in noisy, chaotic, bizarre, and sometimes dangerous environments.
a. Reduce noise and promote a quiet, calm atmosphere.
b. Try not to shout.
c. Talk close to your patient’s ears in a calm voice.
#44 Lecture Outline
4. Therapeutic communication involves the use of specific strategies to encourage the patient to express ideas and feelings.
a. Allows you to convey your respect, acceptance, and genuine concern for someone you have never met before
b. Convince people you want to hear what they have to say.
c. Give them your undivided attention.
d. Pay attention to what patients say.
e. Jot down patient’s responses.
5. Employ active listening.
a. Repeat the key parts of a patient’s response to questions.
#45 Lecture Outline
B. Developing rapport
1. Good rapport with your patient is essential for obtaining good medical information.
2. If patients are reluctant to share personal information:
a. Explain why you need their name and date of birth.
b. Reassure the patients that all information is confidential and protected by law.
3. If patients have trouble focusing, move them safely to the ambulance.
a. Creates a calmer atmosphere
b. Makes talking and listening easier
#46 Lecture Outline
4. If patients feel threatened:
a. Cautiously approach using open postures.
b. Smile and be calm.
c. Reassure the patient.
d. Take things slower if possible.
#47 Lecture Outline
5. Introductions are the first step in promoting open communication.
a. Introduce yourself as soon as possible.
b. Make and maintain eye contact.
c. Get on the same level as the patient.
i. Promotes trust and alleviates anxiety, particularly with children
d. Position yourself so the patient can easily see you.
e. Be aware of body language.
i. Use open-handed gestures.
ii. Do not cross your arms.
iii. Do not react with skepticism.
f. Use the patient’s name in all interactions.
g. Speak slowly and calmly.
h. Always be honest.
#48 Lecture Outline
6. Respect and protect patient’s modesty.
a. This is especially important for older adults, adolescents, and young children.
b. Even if a patient is not personally sensitive to modesty, family members are.
#49 Lecture Outline
C. Conducting the interview
1. There are two types of interview questions:
a. Open-ended questions
i. Allows patients to give you feedback and information
ii. Allows you to judge patient’s mentation
iii. Example open-ended question: “How are you feeling at this moment?”
b. Closed-ended questions
i. Also known as direct questions
ii. Used to elicit a specific answer
iii. Example closed-ended question: “What year were you born?”
2. Always start with open-ended questions.
#50 Lecture Outline
3. Ask one question at a time and let the patients answer at their own pace.
4. Develop a standard set of questions for collecting medical history.
5. Use simple language that people without medical training will understand, but avoid talking down to them.
#51 Lecture Outline
D. Strategies to elicit useful responses to questions
1. Reflection
a. Repeating a word or phrase a patient has used to encourage more detail.
b. This technique can produce more information than the patient originally gave.
2. Empathy
a. Putting yourself in the patient’s position
3. Confrontation
a. This involves making your patients aware that you understand something is inconsistent about their story.
b. Always consider whether this technique could provoke the patient.
c. Remain professional and nonjudgmental.
#52 Lecture Outline
4. Interpretation
a. Vocalize what you think the patient is saying and invite the patient to correct you.
b. This can be used when:
i. You are not sure what a patient is telling you.
ii. A patient refuses to give needed information.
c. Example: If a teenager acts distressed and says she is afraid she might hurt her parents if she tells them what is wrong and says her parents don’t like her boyfriend, you might ask a question like, “This may be totally wrong, but I must ask the question so I can inform the doctor for your well-being. Do you think you are pregnant?”
d. Interpretation requires your best intuition and diplomatic skills.
i. Possible phrase to begin with is, “So if I understand correctly, what you are saying is . . .”
5. Facilitation
a. Use phrases to encourage patients to provide more information.
i. Examples: “Please tell me more about that,” or “What do we need to know about you to be most helpful?”
6. Silence
a. If patients seem to be trying to put something into words, be patient and do not say anything for a few seconds.
#53 Lecture Outline
7. Clarification
a. Ask patients to explain what they mean if you do not understand.
8. Redirection
a. If patients mention something in passing or avoid a certain question, politely redirect their attention to it until you get an answer.
9. Simplification and summarization
a. If the patient’s response is confusing or disorganized, try summarizing his or her comments in simpler terms and see if the patient agrees.
#54 Lecture Outline
E. Common interviewing errors
1. Providing false assurance or making unlikely claims
2. Offering a diagnosis or medical advice that is beyond your scope of practice
3. Asking leading questions
4. Interrupting the patient or talking too much
#55 Lecture Outline
F. Nonverbal skills
1. First impressions are important.
a. Look and act professional at all times to instill confidence.
2. Be patient and calm.
a. Acting impatient will make the patient uncomfortable and stressed.
3. Avoid gestures, facial expressions, and closed postures that send negative signals.
a. Don’t frown or smirk at answers.
b. Maintain constant, nonjudgmental eye contact.
c. Keep your voice calm and neutral.
d. Encourage answers; don’t demand them.
4. Some people do not like to be touched, while it is reassuring to others.
a. Start by touching a shoulder or arm to reassure or reduce anxiety.
b. If they react positively, use touch to help reassure. If not, use other strategies.
#56 Lecture Outline
G. Special interview situations
1. Special communication techniques
a. You may need these techniques with patients who are uncommunicative, hostile or violent, older patients, young children, or those with special challenges.
b. Avoid stereotyping any patient group.
#57 Lecture Outline
2. People who are hostile or violent
a. The heightened emotion of emergency situations can cause patients to become hostile, even toward providers.
b. Acknowledge the hostile person’s concerns.
i. Remain calm and try to understand that person’s concerns.
ii. Use interpretation, clarification, and summarization.
c. You may need to get help from law enforcement to defuse a hostile person.
d. Expect to receive insults from people in crisis, possibly almost daily.
i. Never respond in kind.
ii. Trading insults can escalate a situation.
#58 Lecture Outline
e. Hostile or angry patients may present a threat to you and others.
i. Always approach with caution, maintaining eye contact.
ii. Avoid interviewing an angry patient by yourself.
iii. Have law enforcement personnel or other EMS responders close by as backup.
iv. Identify escape routes from the scene.
v. Approach the patient from the front, with hands visible and open.
vi. Introduce yourself, explain your role, and ask for the patient’s name.
#59 Lecture Outline
vii. If safe, get on the patient’s level.
viii. Ask permission to ask questions and touch the patient.
ix. Always be honest.
x. Be wary for signs of impending attack, such as clenched fists, hostile language, tensed neck and face muscles, and threatening gestures.
#60 Lecture Outline
3. Sexually aggressive patients
a. Occasionally, you will encounter sexually aggressive patients.
b. Make sure a second person is always present when you are with the patient.
c. Communicate professionally and politely.
d. Make sure your words are not sexually ambiguous.
e. Most of all, maintain professionalism at all times.
f. Follow your agency’s policies, document your encounter, and get witness names and signatures.
#61 Lecture Outline
4. Special considerations of age
a. Older people
i. Don’t assume older people are harder to communicate with than others.
ii. Older people tend to have more complex illnesses because they may have multiple diseases or conditions.
iii. Older people may be taking several kinds of medications.
iv. Members of the older adult population have individual differences related to hearing, eyesight, mentation, and mobility, to which you may need to adapt.
b. Children
i. Children tend to protest pain vigorously.
ii. They may be afraid of strangers.
iii. They can panic when separated from their parents or caregivers.
iv. Their bodies may be unfamiliar; practice may be needed for you to become comfortable with simple procedures.
#62 Lecture Outline
v. Tips for communicating with small children include:
(a) Use friendly eye contact, smiles, and calm explanations.
(b) Minimize movements, lower your voice, and touch gently.
(c) Start by talking with the patient’s parent or caregiver.
(d) Keep eye level at or below child’s level.
(e) Involve parent in hands-on care, especially with infants and toddlers.
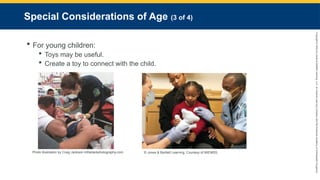
(f) In the absence of parents, toys such as teddy bears may be helpful.
#63 Lecture Outline
(f) In the absence of parents, toys such as teddy bears may be helpful.
#64 Lecture Outline
c. Adolescents
i. Generally, deal with adolescents as adults, offering realistic options and choices.
ii. Children age 13 and above may not want parents or caregivers present during exams.
iii. Protect modesty of any children over age 2, particularly adolescents.
iv. Avoid disrobing patients unless necessary.
#65 Lecture Outline
5. People with special challenges
a. When you encounter a patient who has trouble communicating, remember that family members or caregivers can facilitate your efforts.
b. Caregivers may take classes in sign language or lip reading to aid communication.
c. Help patient access their glasses, hearing aids, or other devices that might help communication or reduce fears.
d. Touch and eye contact may help convey kindness or reassurance.
i. Example: A light touch on a shoulder or a brief one-armed hug
#66 Lecture Outline
e. Pervasive developmental disorders (PDDs), such as autism, cause delays in childhood development and may have lifelong effects.
i. Children with autism may have difficulty with language skills.
ii. They may also have difficulty communicating nonverbally.
iii. People with PDDs range widely in skill development, from being unable to speak to having problems with meaning.
iv. Communicate with patients with PDDs through a caregiver if possible.
#67 Lecture Outline
VIII. Cross-Cultural Communication
A. Cultural competence
1. Ethnocentrism is the belief that one’s own culture or ethnic group is inherently superior to others, or that one’s own cultural viewpoint is always right, while others’ viewpoints are wrong.
a. Can lead to incorrect assumptions
2. Cultural competence may interfere with your ability to provide appropriate emergency medical care because you have misinterpreted information.
#68 Lecture Outline
3. Be aware that cultures and religions may have certain beliefs that conflict with standard medical procedures, such as the use of oxygen.
a. The culturally competent response is to try to understand why the patient is reacting in a manner you did not anticipate.
#69 Lecture Outline
4. Culture can be defined as the system of beliefs, attitudes, and behaviors that are learned and shared by members of a group.
a. Human beings are not born with a sense of culture; it is learned from others.
i. Every person you encounter has a mixture of cultural influences that will impact how they behave and how they will behave when stressful situations arise.
ii. It is your responsibility to recognize these differences and to understand how they may affect your interactions with the diverse population you serve.
(a) This is referred to as cultural competence.
#70 Lecture Outline
B. Cultural awareness
1. Body language
a. Body language may also be interpreted differently by different cultures.
b. The smile is used almost universally as a sign of goodwill.
c. The following is a list of some cultural practices paramedics should be aware of:
i. Eye contact: Avoiding direct eye contact is a sign of respect in some Native American, Asian, African, Latin American, and Caribbean cultures. Prolonged eye contact is acceptable in the Arab world, Somalia, Brazil, and most European cultures.
ii. Touching with the left hand: Islamic and Hindu cultures avoid touching with the left hand; it is considered rude to use the left hand in greeting.
iii. Touching the head: Many Asians do not touch the head as it is considered the most sacred part of the body.
iv. Feet: Showing the bottom of the feet is offensive in Muslim nations and most of Thailand.
v. Hands on hips: This can convey hostility in Mexico and Argentina.
vi. Nodding: Indian and Arab cultures may signal agreement by moving head side to side (the Western “no”); some members of Asian cultures will nod to acknowledge that someone is speaking, but that gesture does not indicate agreement.
vii. Hand gestures: These can have very different meanings in different cultures. Some gestures may be innocent to one cultural group but insulting to another. Learn about and be cautious with your use of hand gestures with those from different cultures in your community.
#71 Lecture Outline
C. Traditional folk medicine and understanding of illness
1. Many immigrants to the United States follow the traditional folk medicine practices of their culture or homeland.
2. Traditional models of illness typically involve a belief that health is the result of balance of forces.
a. Treatments and remedies are aimed at restoring the balance.
b. Some beliefs may view the illness as a result of the loss of one’s spirit or of magical influences.
3. Some humoral medicine practices have regained popularity among followers of the New Age movement.
a. Immigrants and the children of immigrants may practice a blend of Western and traditional health practices.
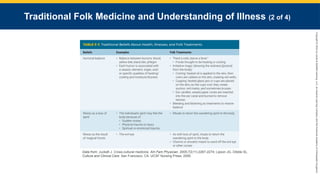
#72 This table shows a few traditional beliefs about health, illnesses, and folk treatments.
#73 Lecture Outline
b. Cupping and coining are two folk medicine practices that you must be aware of because they may be easily misinterpreted as signs of physical abuse.
4. The use of herbal medications is another area of traditional folk medicine.
a. Many herbal medications have significant pharmacologic effects that may be a source of the patient’s symptoms, or they may interact with other prescribed medications.
b. Patients may be taking medications brought from their native country or supplied by family members.
c. Collect all of the patient’s medicines and bring them to the hospital so they can be identified.
#74 Lecture Outline
5. Some patients may not share the beliefs of their families or cultural backgrounds.
a. Always remain sensitive to the patient’s individual religious, cultural, and sociological beliefs.
#75 Lecture Outline
D. Language Interpretation
1. The most significant communication challenge with members of other cultures is lack of a common language.
a. It may be impossible to perform a good history and assessment.
b. Use a qualified interpreter if possible.
c. When dealing with a patient who speaks another language, you should always assume you are missing something important in your history and assessment and act accordingly.


















![Chapter 015[1]](https://cdn.slidesharecdn.com/ss_thumbnails/chapter0151-120508224443-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)








































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)


![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)



