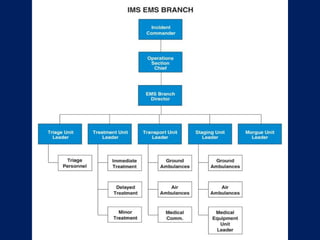
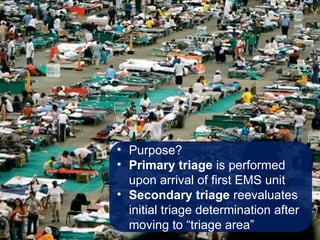
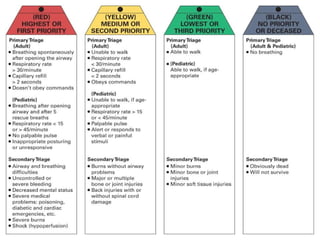
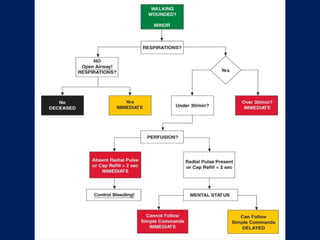
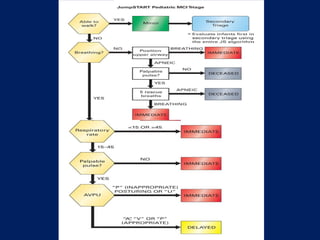
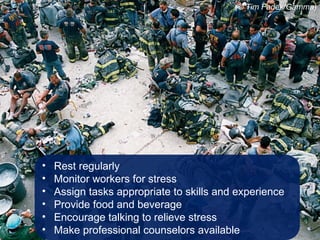
This document discusses the management of multiple-casualty incidents (MCIs) and emphasizes the importance of preparedness and effective communication among responders. It covers key principles of the National Incident Management System (NIMS) and the Incident Command System (ICS), detailing processes such as triage, treatment prioritization, transportation, and post-incident support. Strategies for psychological care of both patients and responders are also outlined, addressing age-specific reactions and the need for accurate communication with families.