Downloaded 62 times



![Signs and Symptoms:Signs and Symptoms:
2. Accommodation fatigue (AF)2. Accommodation fatigue (AF)
Blurred vision after prolonged near work
Accommodative system fails to sustain
accommodation
S& S ]
– Like Acc. Insufficiency
– except Amp.Acc. is normal
Amp. Acc. on repeated testing reduces
Usually fails flipper test (+/- 2.00D)
Decreased PRA](https://image.slidesharecdn.com/accommodativeandvergencedysfunction-190516051542/85/Accommodative-and-vergence-dysfunction-15-320.jpg)


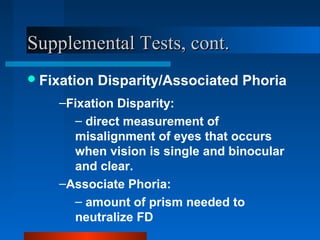

Accommodative and vergence dysfunctions can cause symptoms like blurred vision, difficulty reading, and asthenopia. Key diagnostic tests include cover test, versions, near point of convergence, and fusional vergence amplitudes. Accommodative issues include insufficiency, fatigue, and infacility. Vergence issues include convergence insufficiency, divergence excess, and basic exophoria. Early treatment is important to prevent amblyopia or learning problems from vergence anomalies.




















































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)

