1. Pseudostrabismus is when there is an appearance of eye misalignment but no actual squint, caused by factors like abnormal angles between the visual and anatomical eye axes.
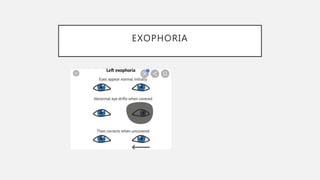
2. Heterophoria is a latent eye misalignment that becomes manifest when fusion is suspended, and can be esophoria (convergent) or exophoria (divergent).
3. Convergence insufficiency, accommodation insufficiency, divergence insufficiency and near reflex insufficiency are different vergence and accommodation abnormalities that can cause visual symptoms and are treated with exercises and lenses.