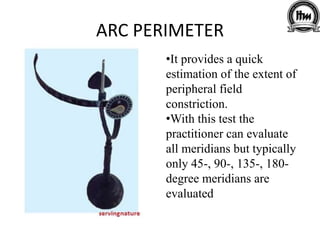
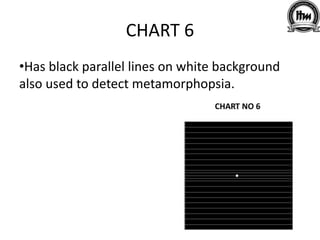
The document discusses low vision and the importance of visual field assessment in patients with visual impairments. It outlines definitions, assessment methods, and the impact of various ocular diseases on visual fields, as well as the implications of visual field loss on occupations. Additionally, it highlights different tools and tests used for evaluating visual fields, including perimeters and grids.
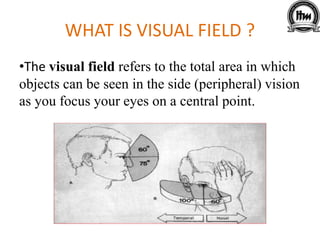
































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




