Downloaded 506 times






















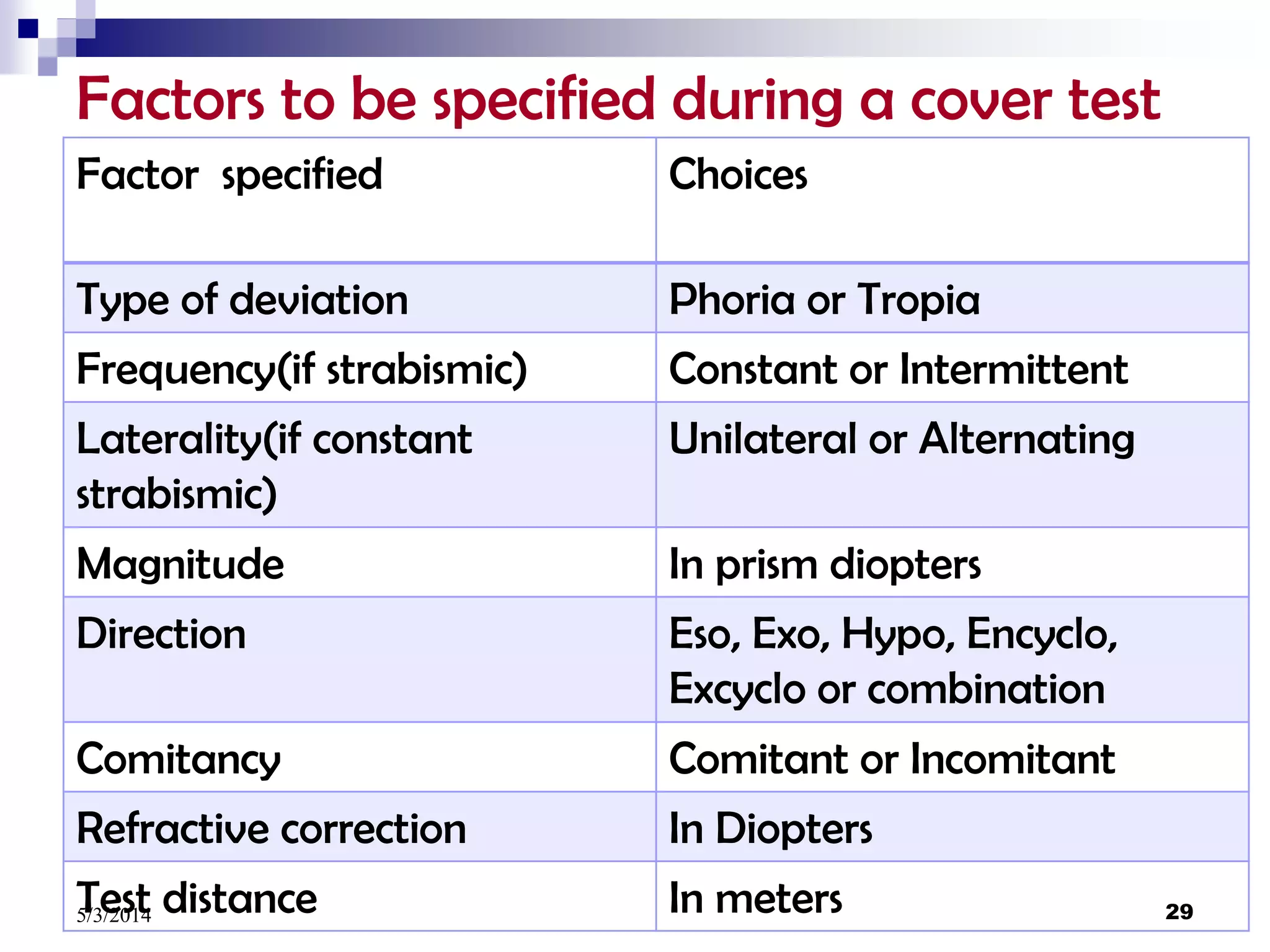

















































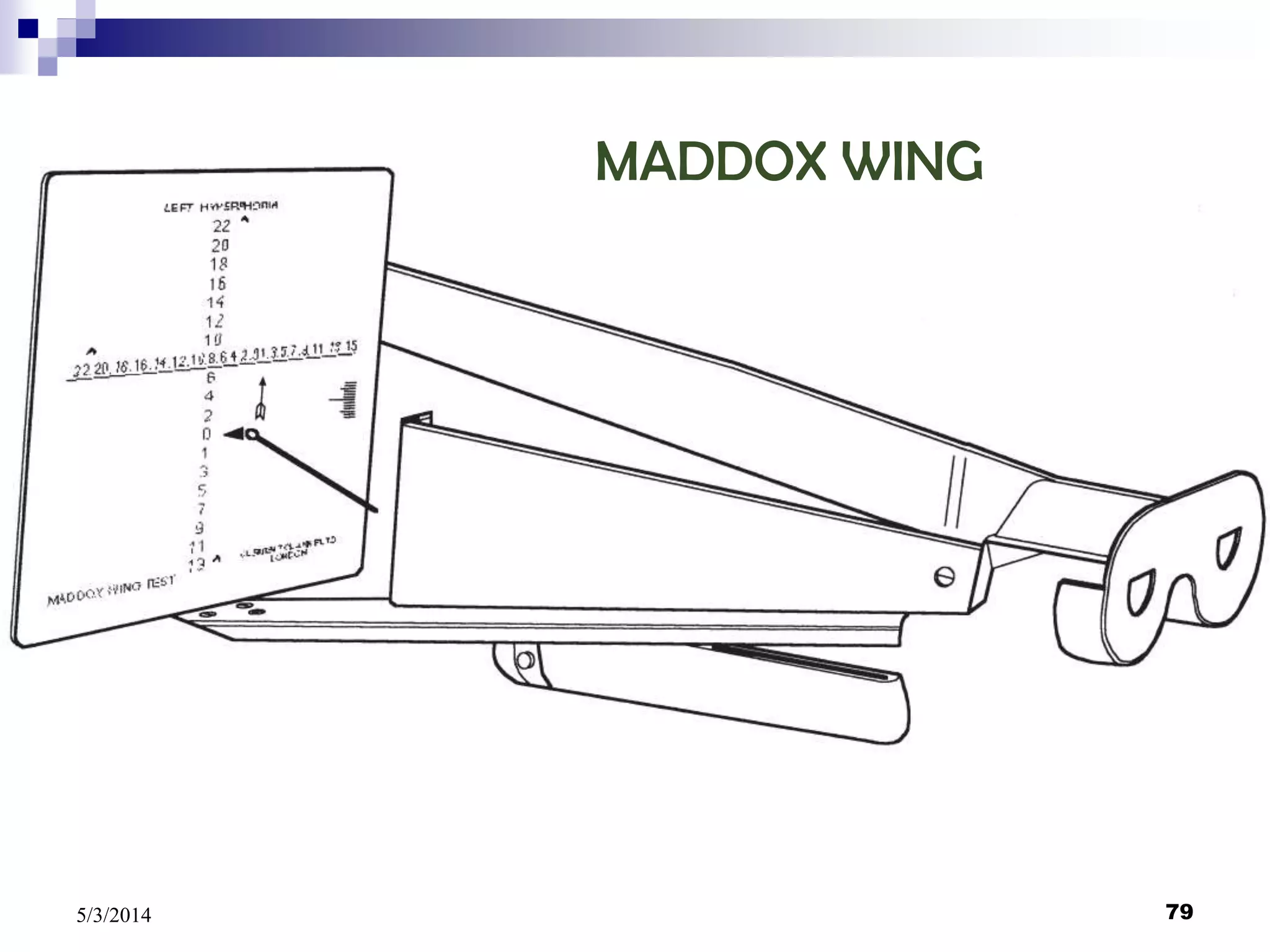




















This document discusses the measurement of heterophoria and heterotropia. It begins with introducing heterophoria as a latent strabismus where the eyes are normally directed to the point of fixation but deviate when dissociated. It then discusses the detection of phoria and tropia through examining the position of the globes and observing head position. Next, it describes determining the presence of a deviation using cover tests and measuring the deviation using objective methods like the prism and cover test and major amblyoscope as well as subjective methods.























































































