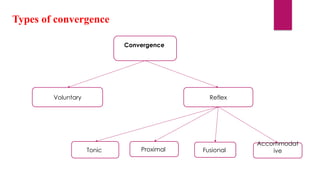
The document discusses the concept of convergence in vision, detailing various types such as tonic, fusional, accommodative, and proximal convergence, along with their functions and anomalies. Convergence insufficiency is identified as a common condition causing ocular asthenopia, characterized by symptoms like eyestrain and blurred vision, and it is diagnosed based on specific metrics and features. Treatment options range from optical interventions to orthoptic exercises and, in rare cases, surgery.




























































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)









