Downloaded 52 times



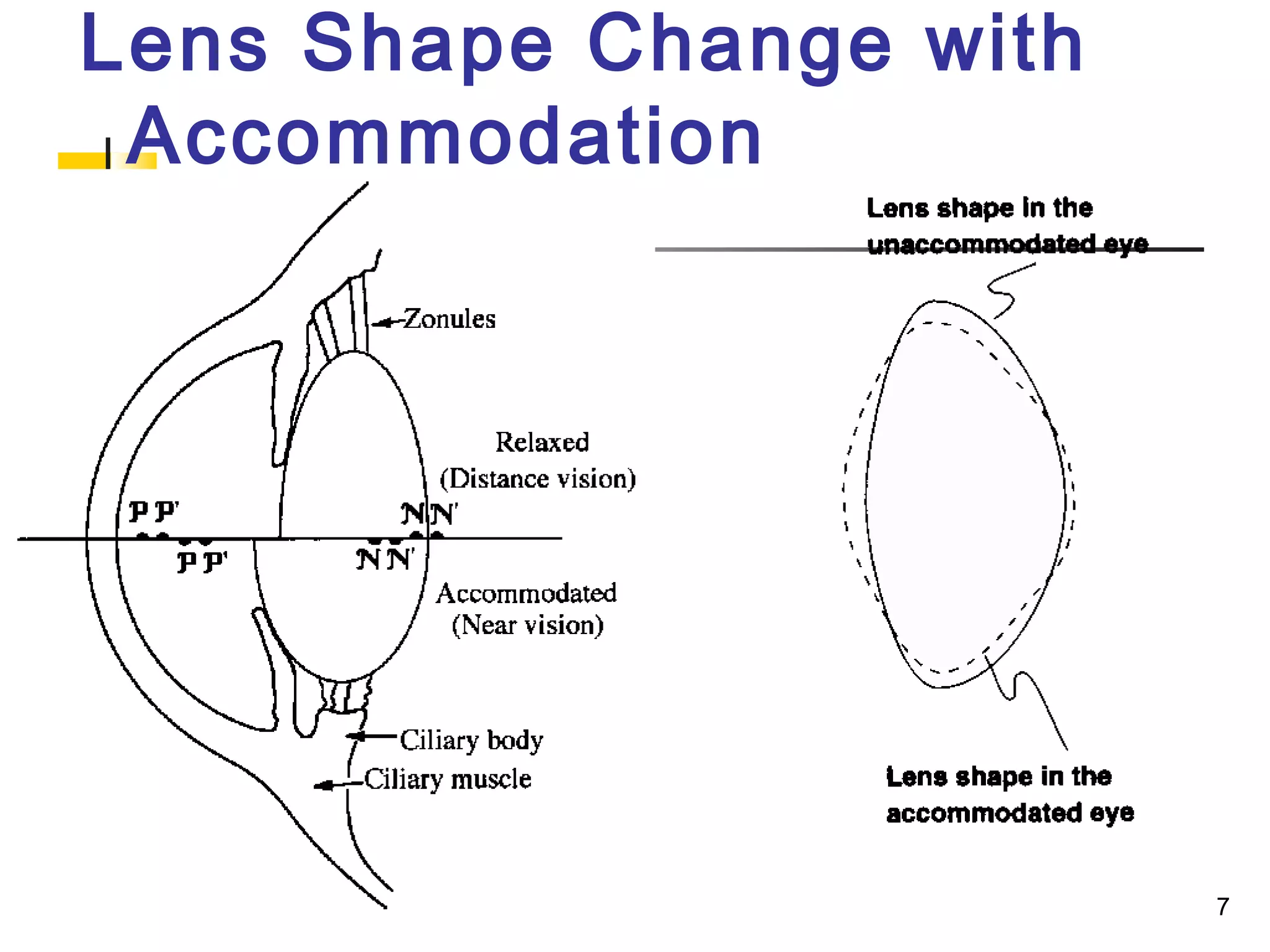








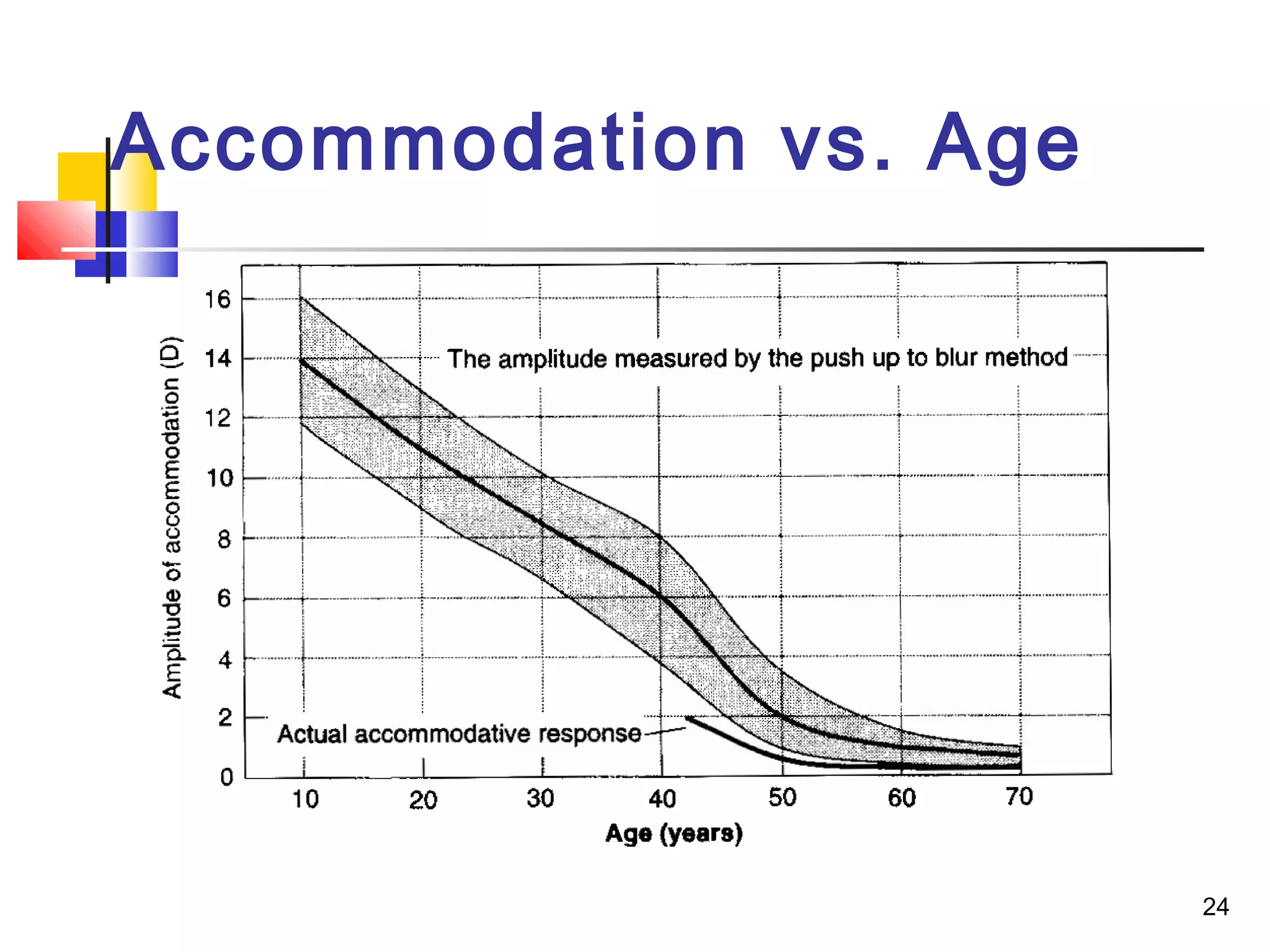
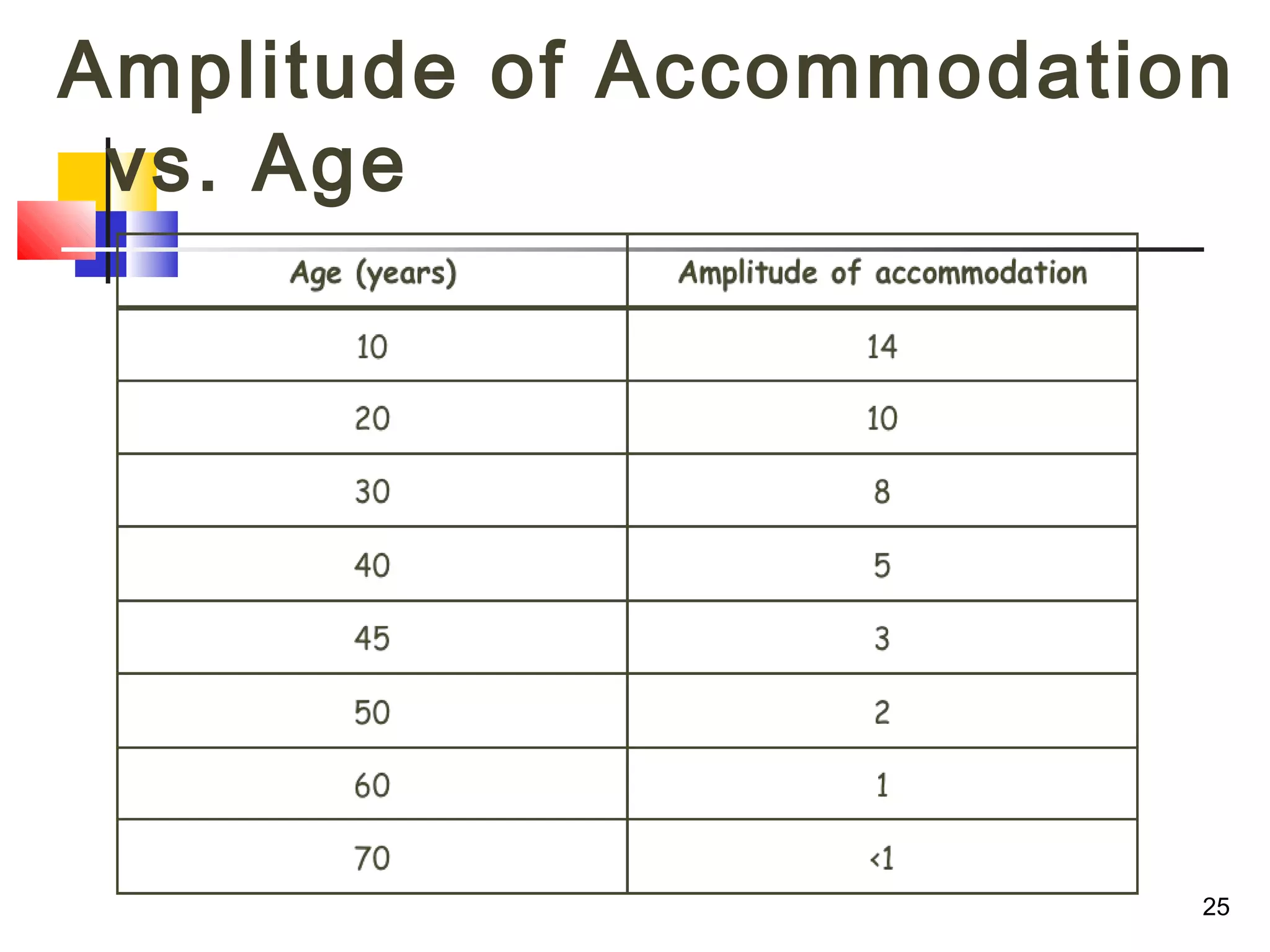
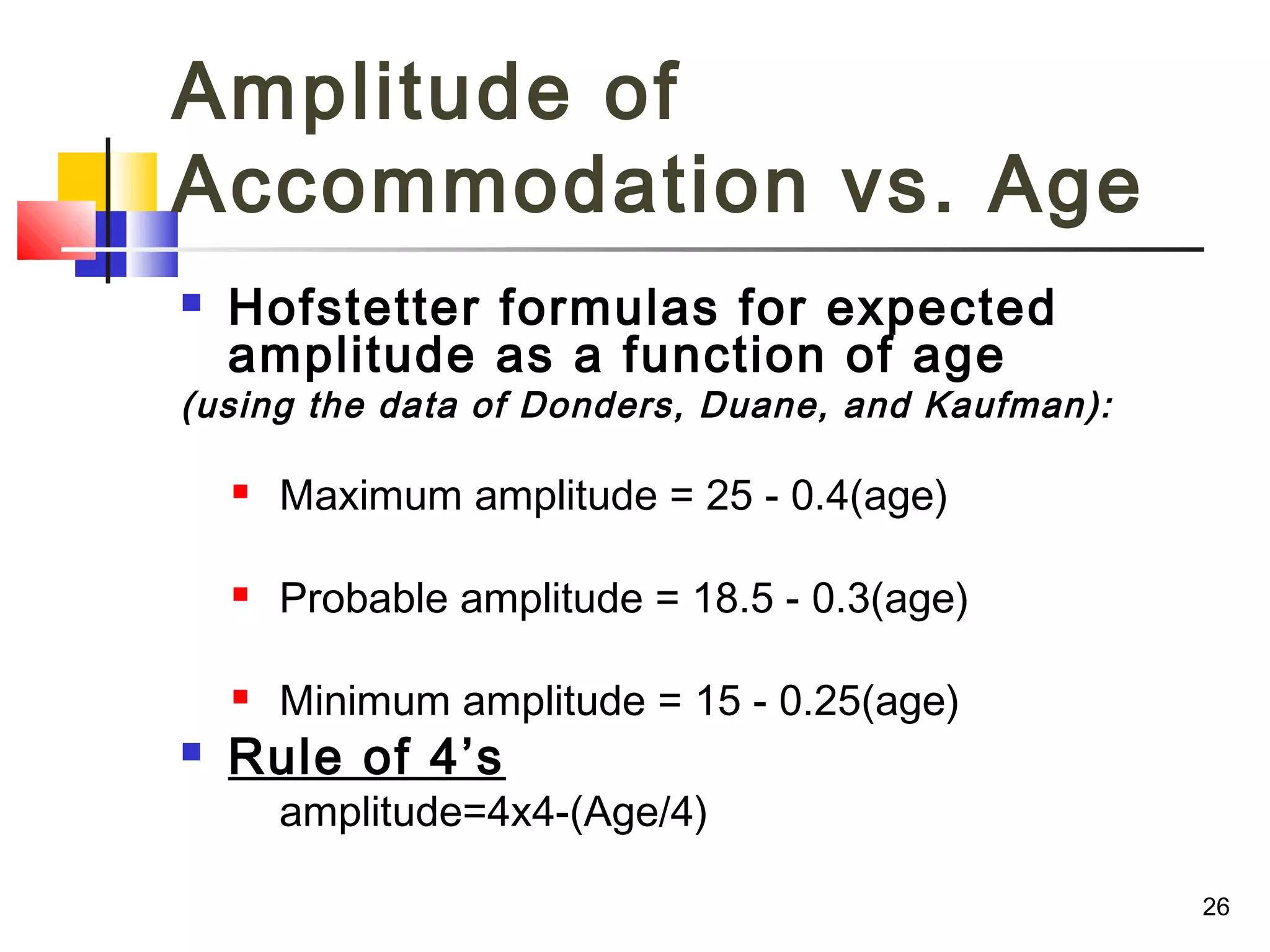









The document discusses various aspects of accommodation including its definition, physiology, components, anomalies, and age-related changes. It defines accommodation as the process by which the crystalline lens changes its power to focus on near versus distant objects. The amount of accommodation depends on factors like age and training. Accommodation is mediated by the parasympathetic nervous system. Anomalies of accommodation include insufficiency, infacility, fatigue, latent hyperopia, spasm, and presbyopia which is the age-related decline in accommodation leading to the need for reading glasses.










































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)











