Downloaded 110 times


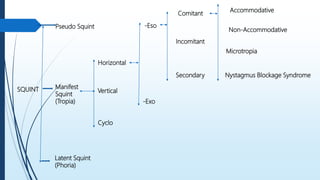
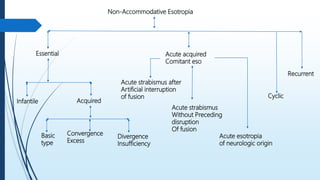










The document provides an in-depth analysis of non-accommodative esotropia, detailing its classification, characteristics, clinical features, and treatment options. It addresses various forms of esotropia, including essential infantile, acquired, and acute acquired, along with specific nuances such as convergence excess and divergence insufficiency. Treatment primarily involves muscle surgery, with consideration for patients' individual circumstances and potential associated factors.



































































