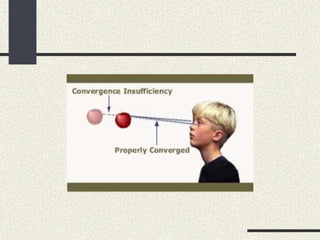
This document discusses convergence insufficiency (CI), including its definition, causes, symptoms, diagnosis, and treatment. CI is characterized by a weak ability to maintain proper binocular eye alignment for near vision tasks. It is often associated with exophoria and reduced fusional convergence. Symptoms include eyestrain, headaches, and blurred vision when reading. Treatment involves orthoptic exercises to strengthen convergence, as well as base-in prisms or surgery in severe cases. The document provides detailed explanations of CI and outlines goals and aspects of its medical, surgical, and follow-up management.