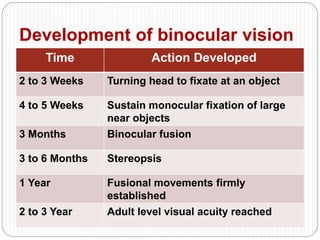
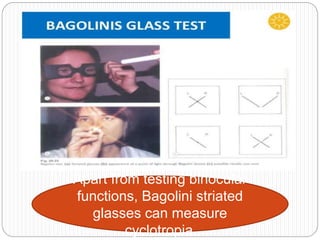
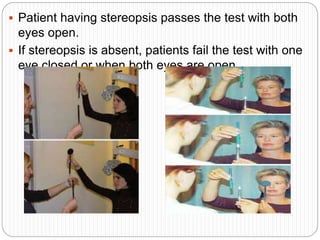
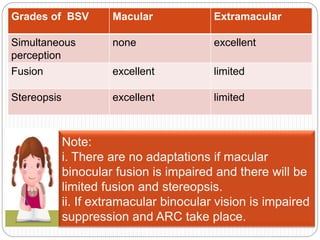
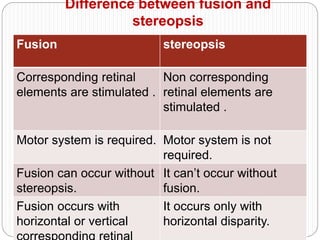
This document discusses measurement of fusion and stereopsis in binocular vision. It begins by defining binocular vision and binocular single vision. It then discusses various classifications, prerequisites, advantages, and related terms of binocular single vision. The document also describes different tests used to measure fusion, including the synaptophore, prism fusion test, Worth's four dot test, Bagolini's striated glass test, and Maddox rod test. It provides details on the procedures and interpretations of these tests. Finally, it discusses the development and grades of binocular vision.