Downloaded 35 times
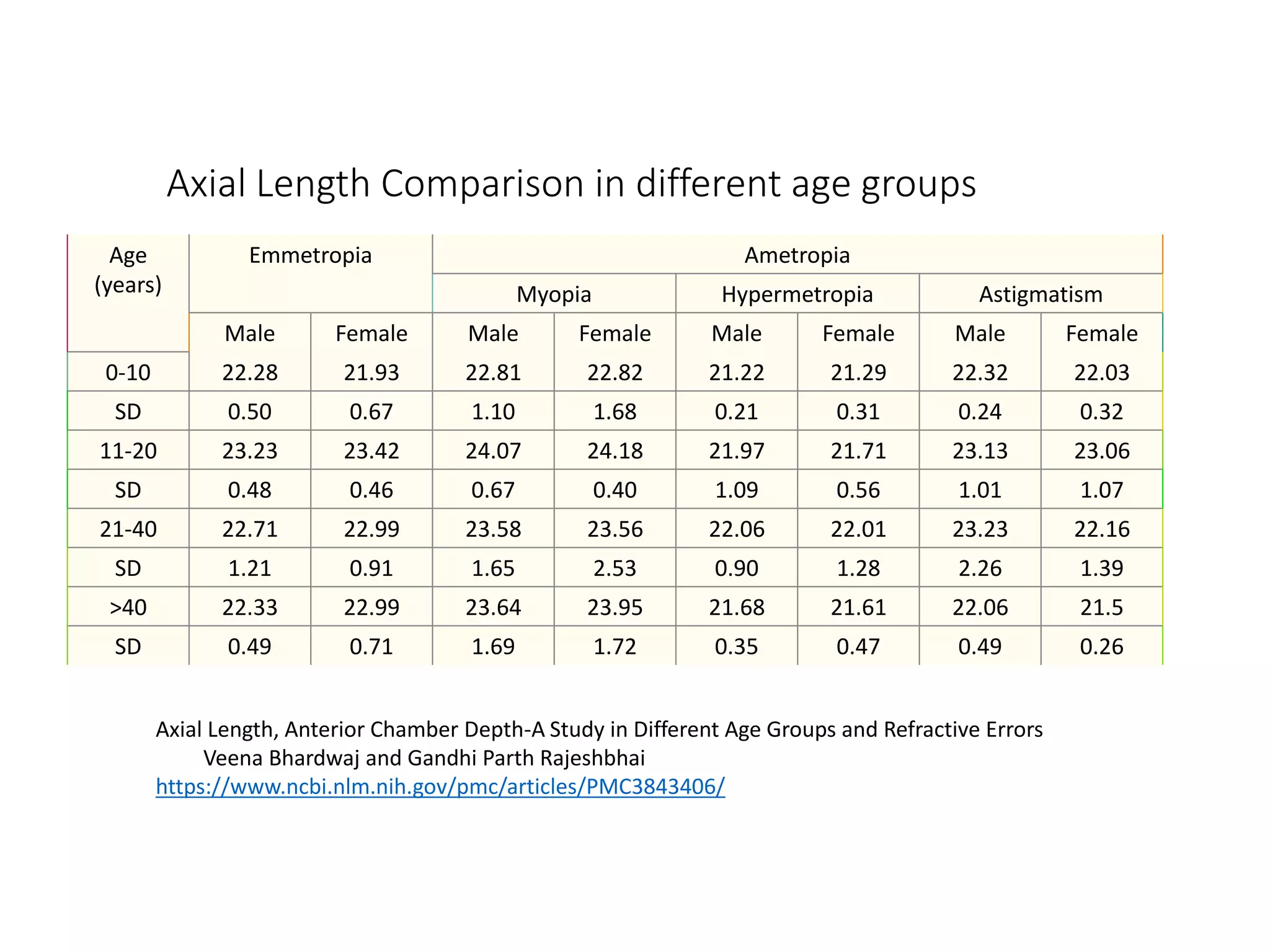
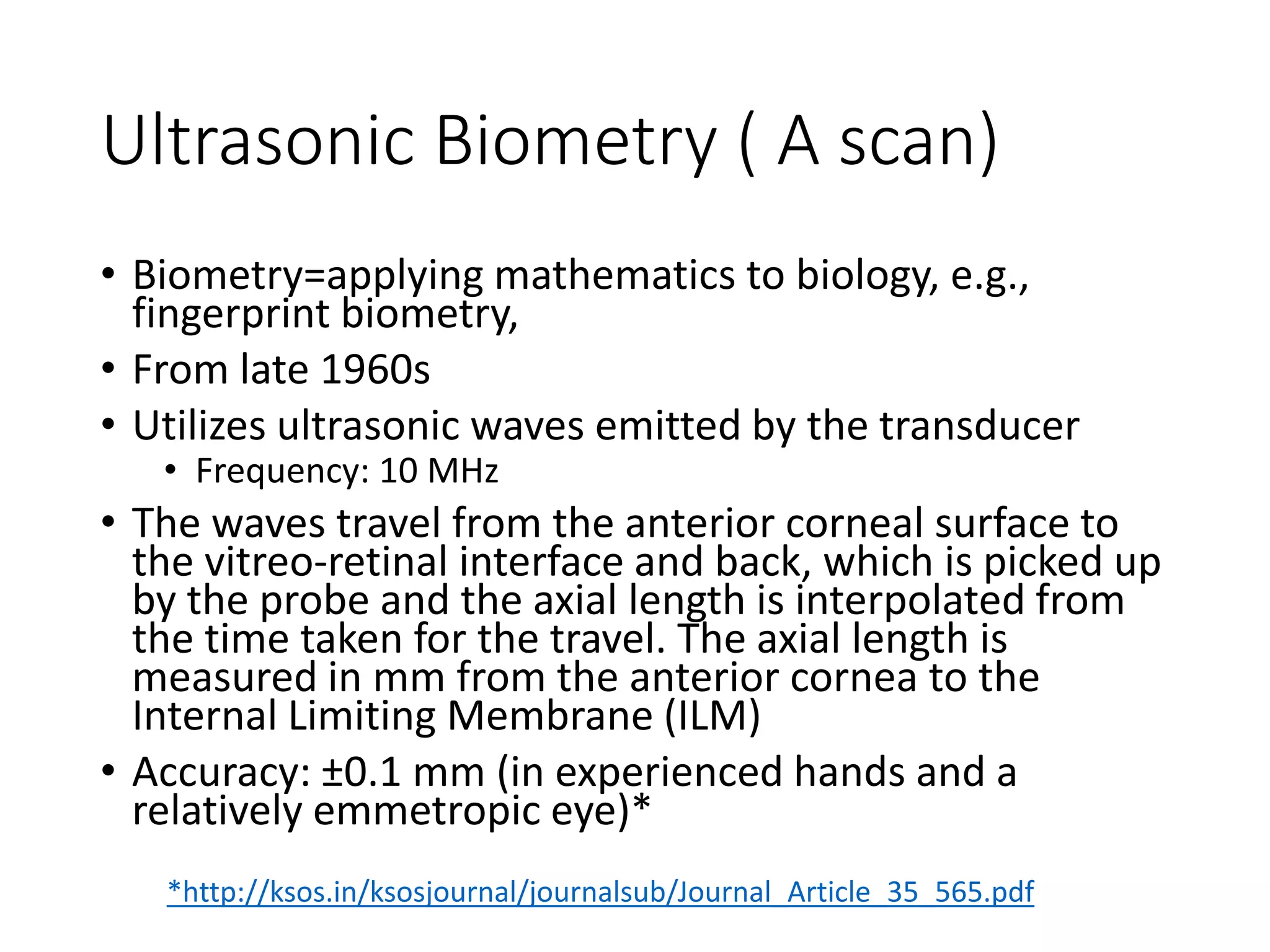
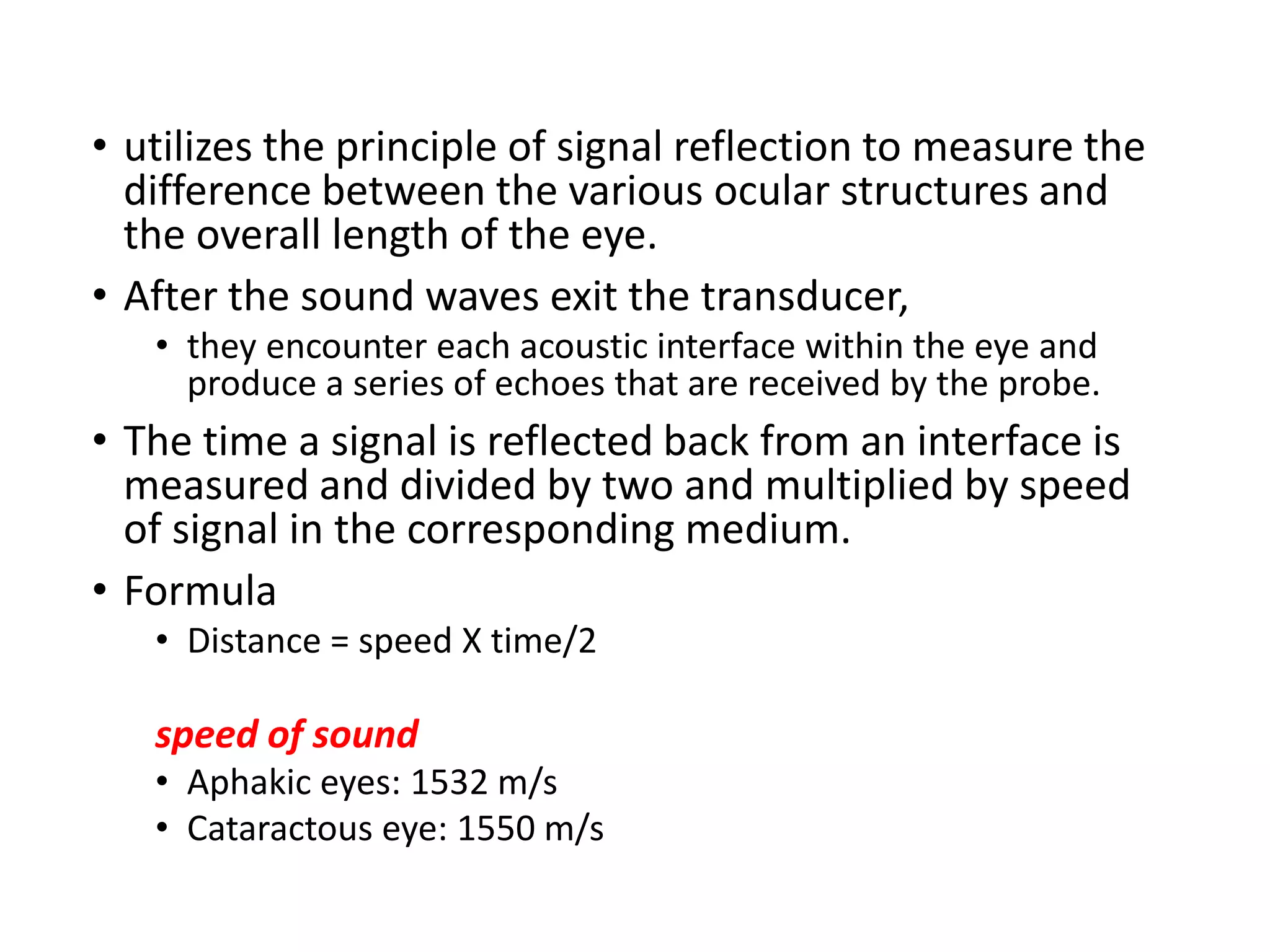
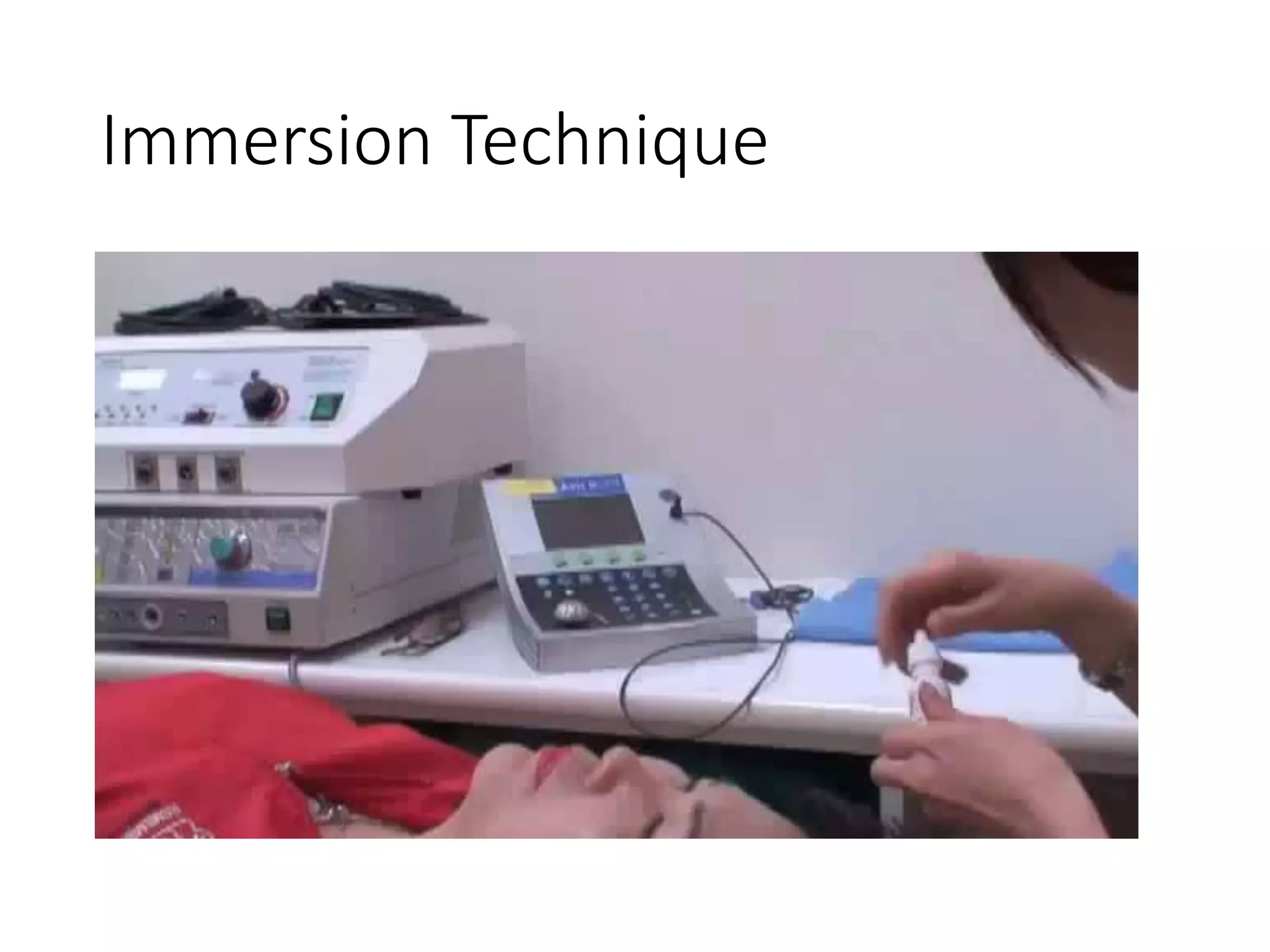
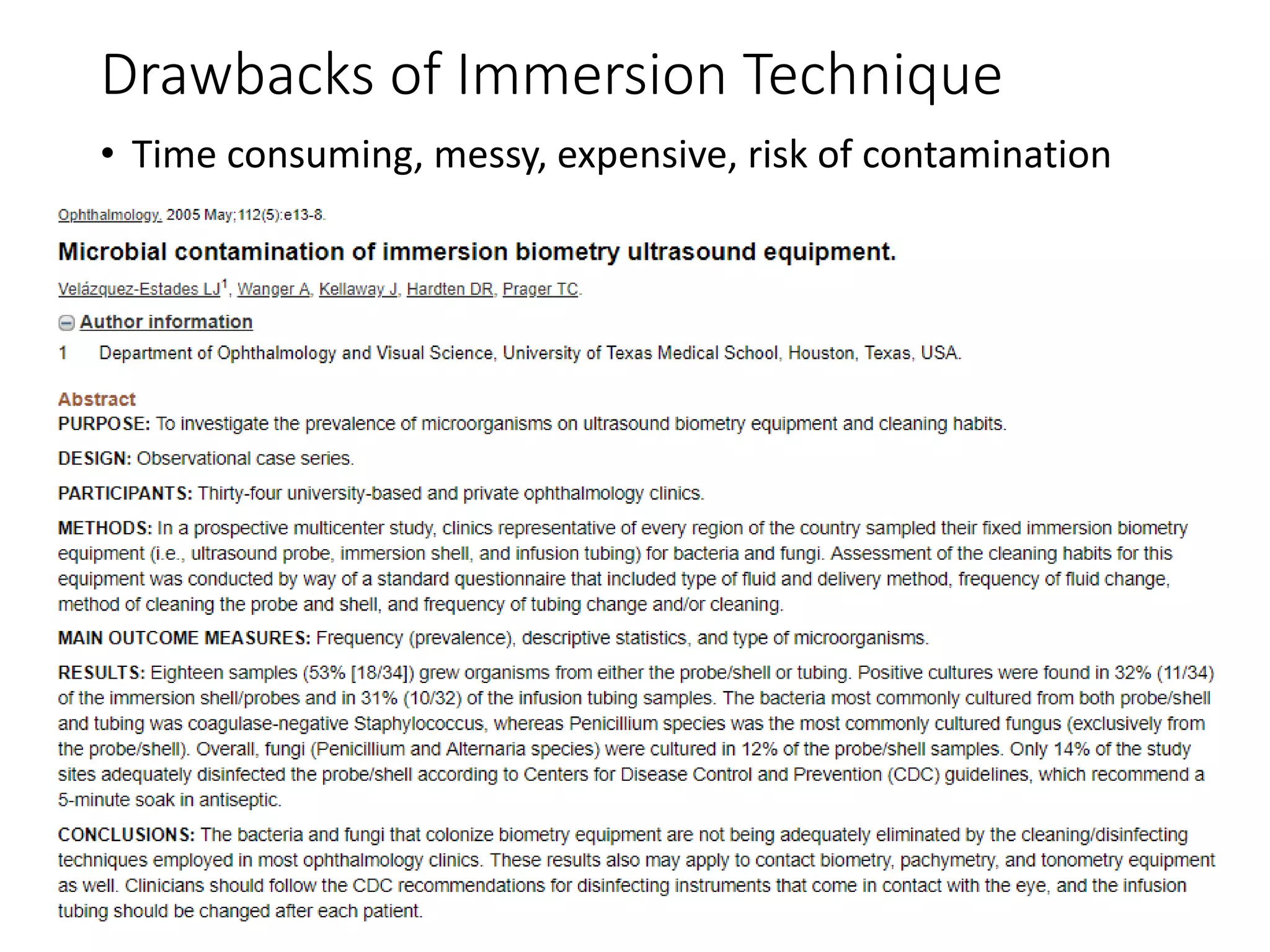
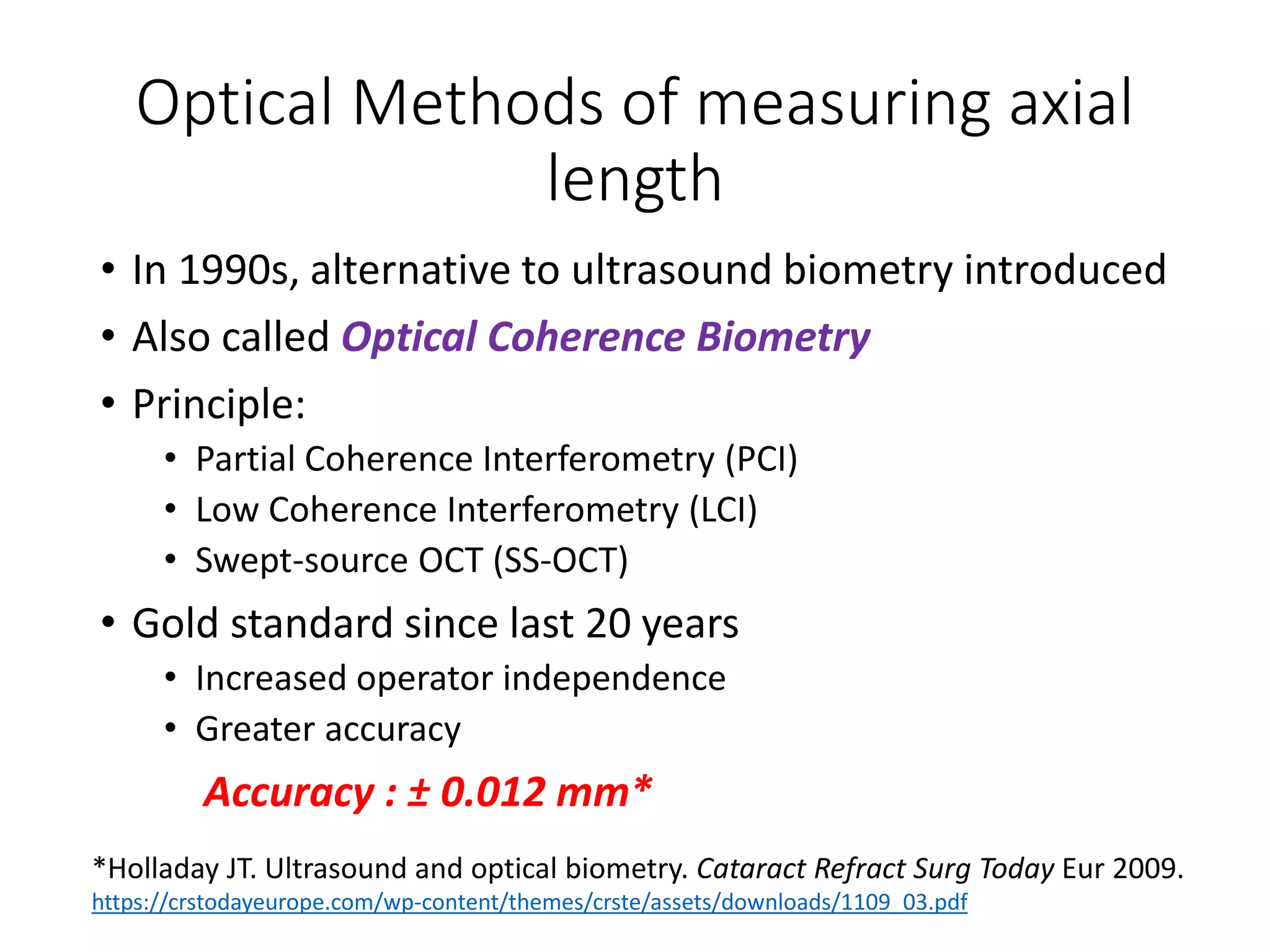
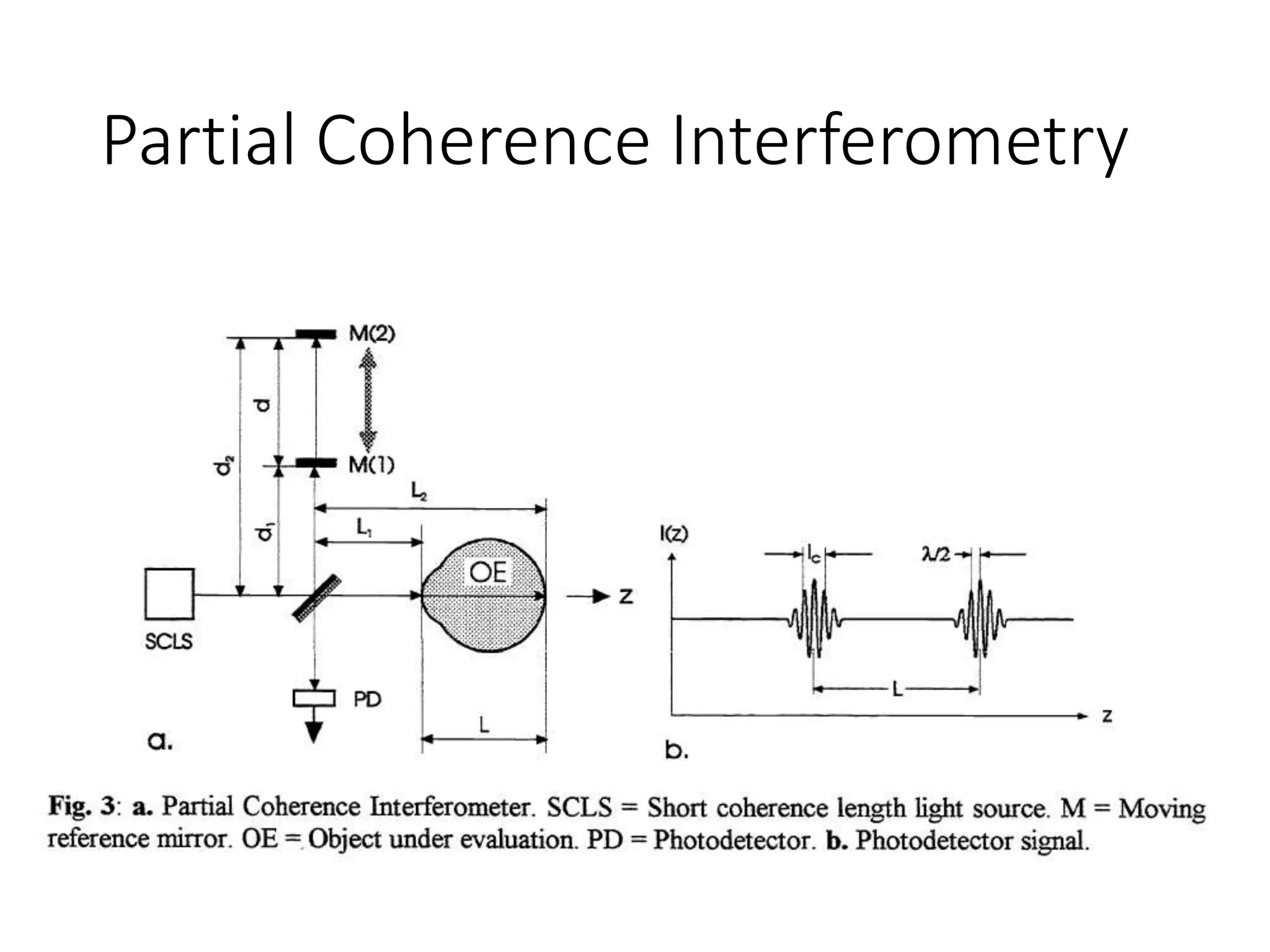
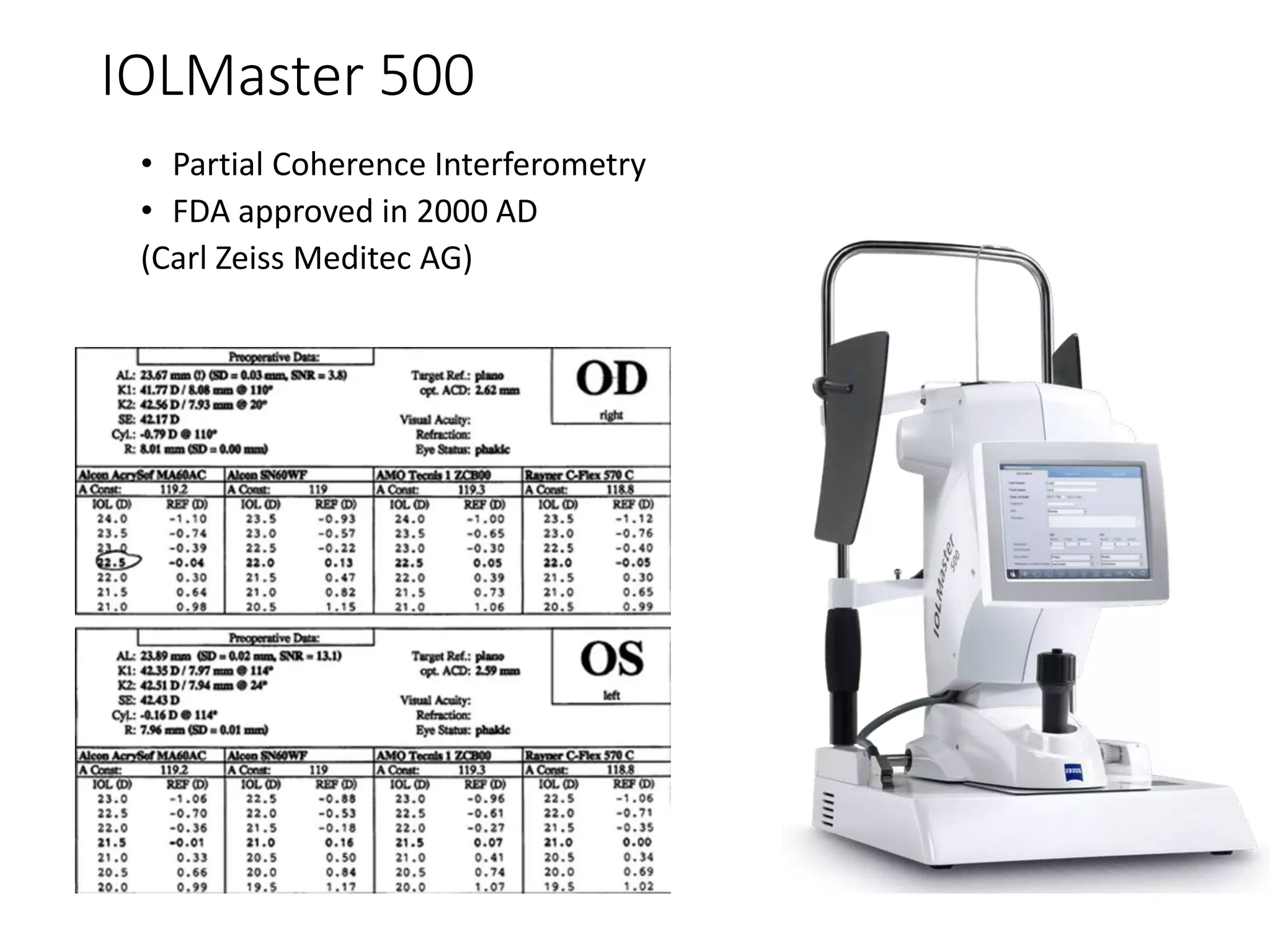
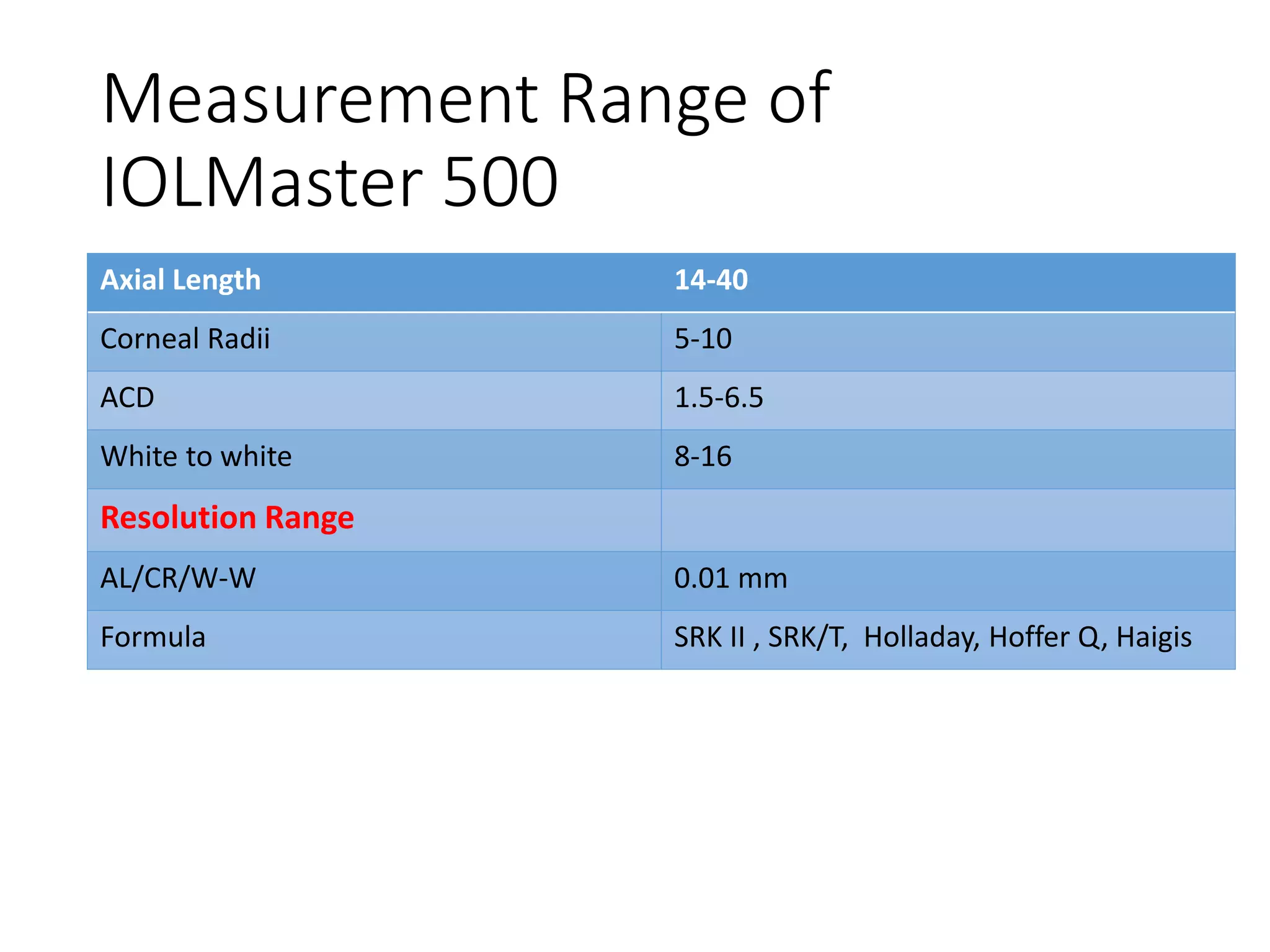
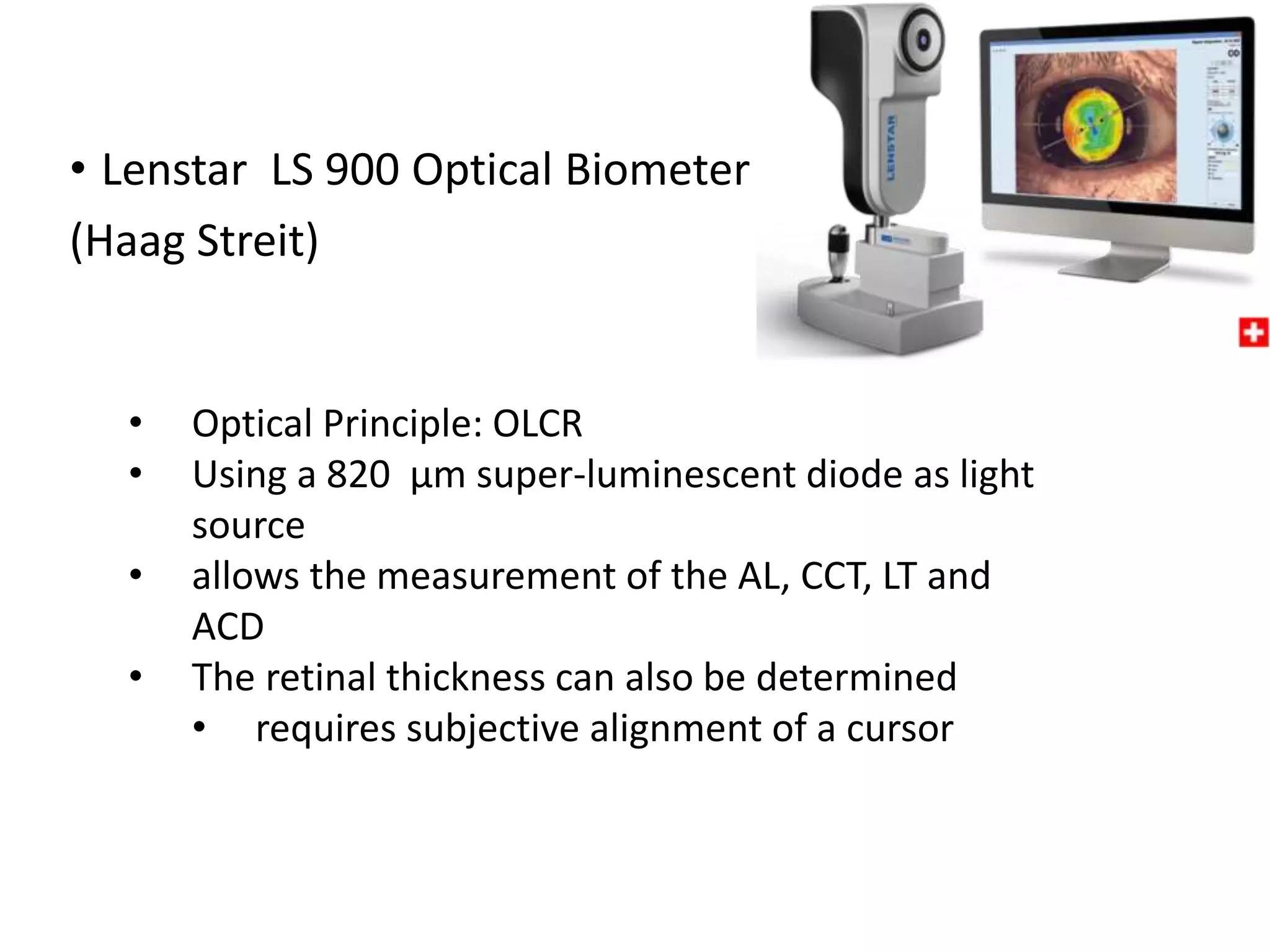

This document discusses various optical and non-optical methods of measuring axial length of the eye. It begins by defining axial length and noting its importance in intraocular lens power calculations. It then describes ultrasonic (A-scan) biometry, the historical standard, and optical biometry techniques like partial coherence interferometry used in devices like the IOLMaster 500. Key advantages of optical techniques are discussed as well as limitations of ultrasound. Details are provided on performing both immersion and non-immersion ultrasound techniques and interpreting the results.