The document summarizes India's national leprosy control programs from 1955 to the present. Key points include:
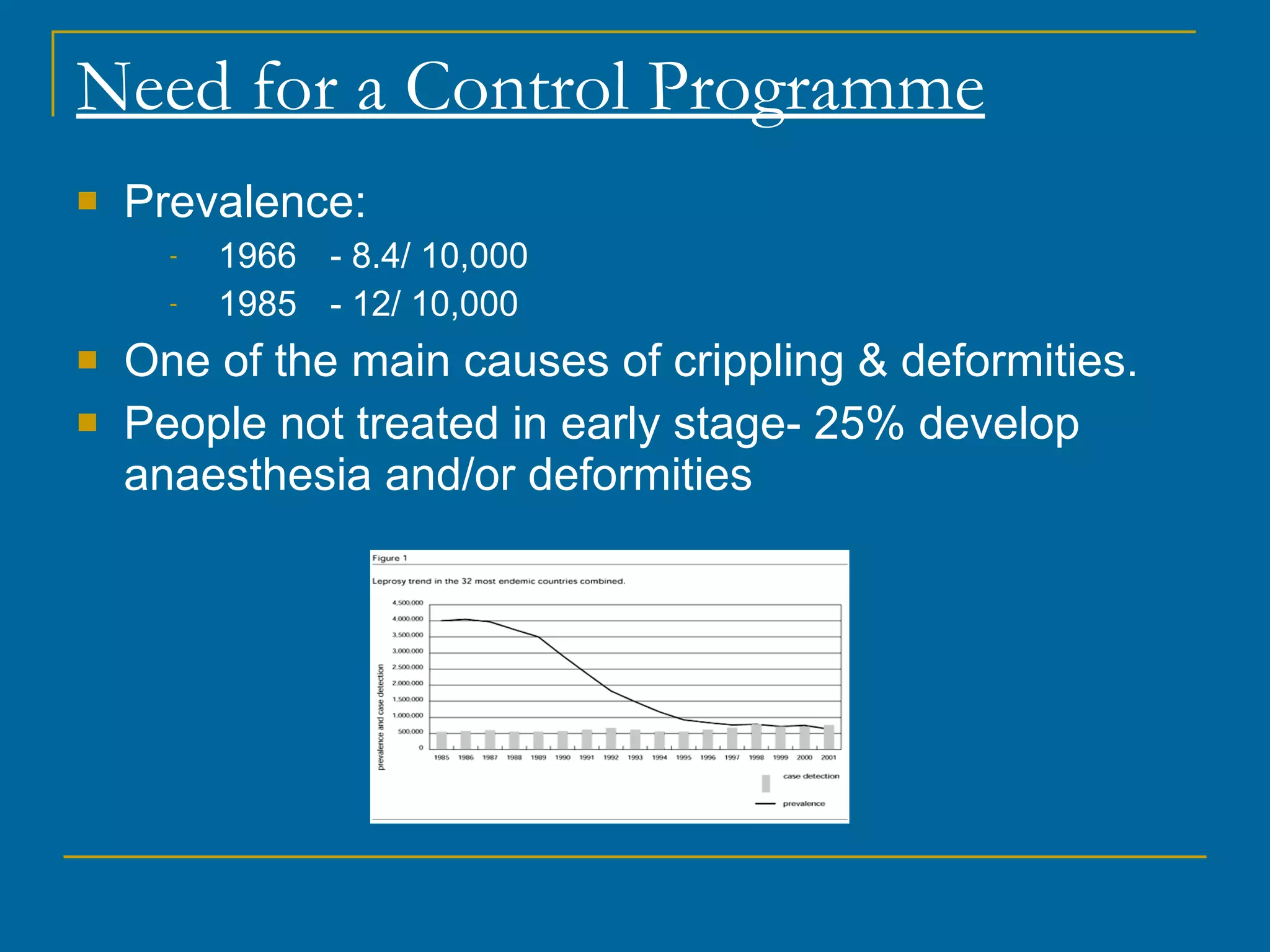
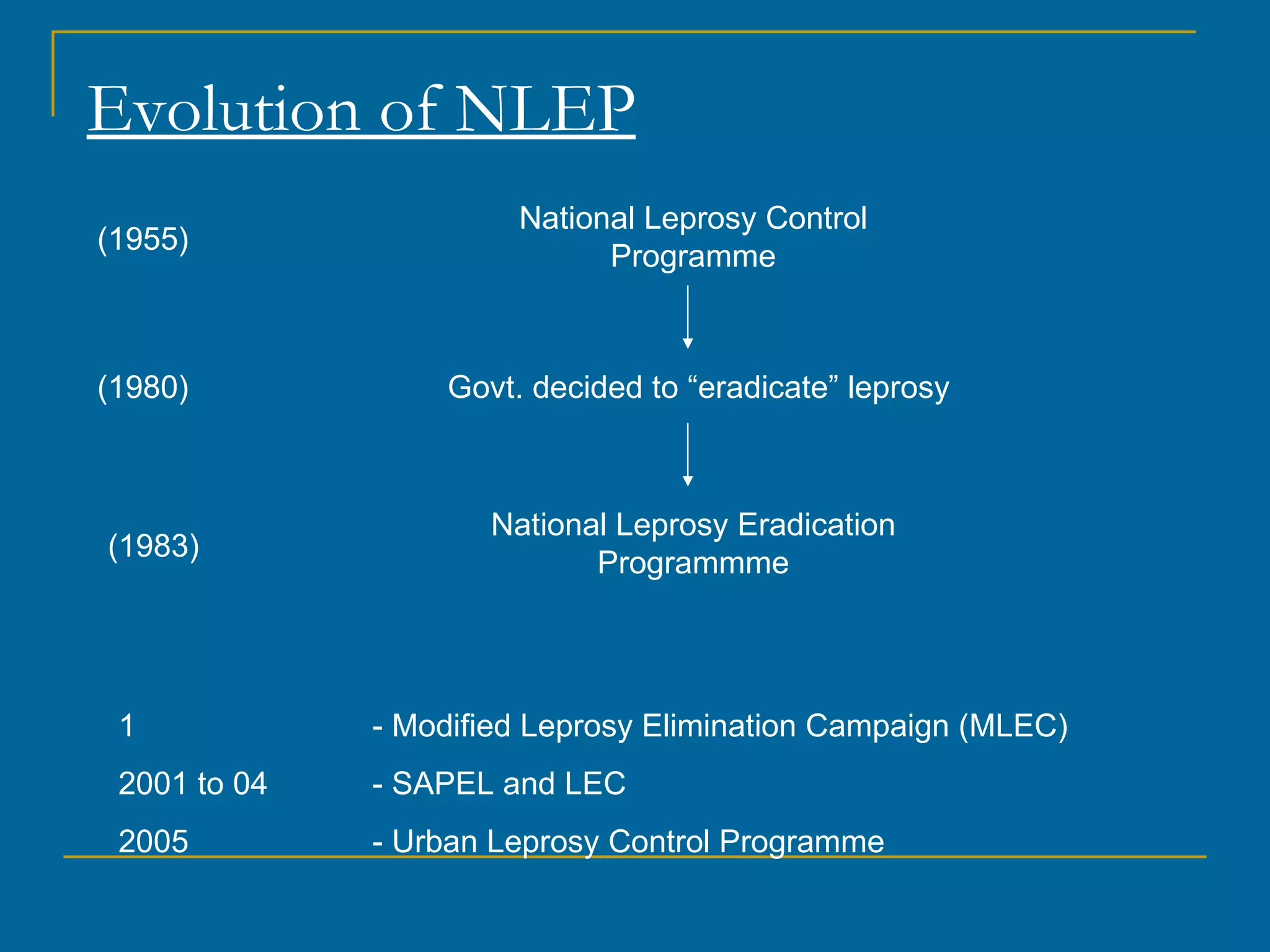
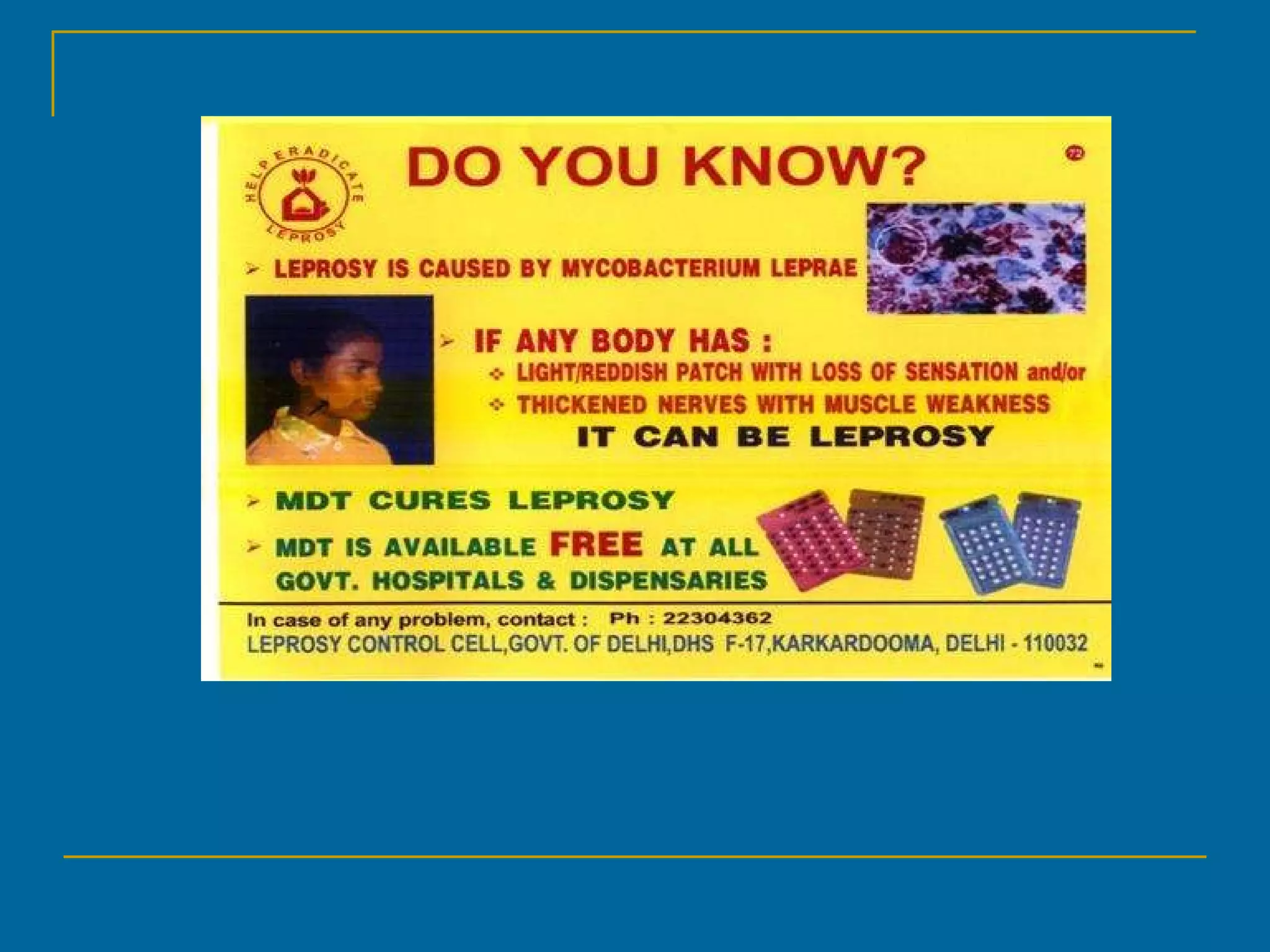
- The National Leprosy Control Programme was established in 1955 to control leprosy through early detection and dapsone monotherapy.
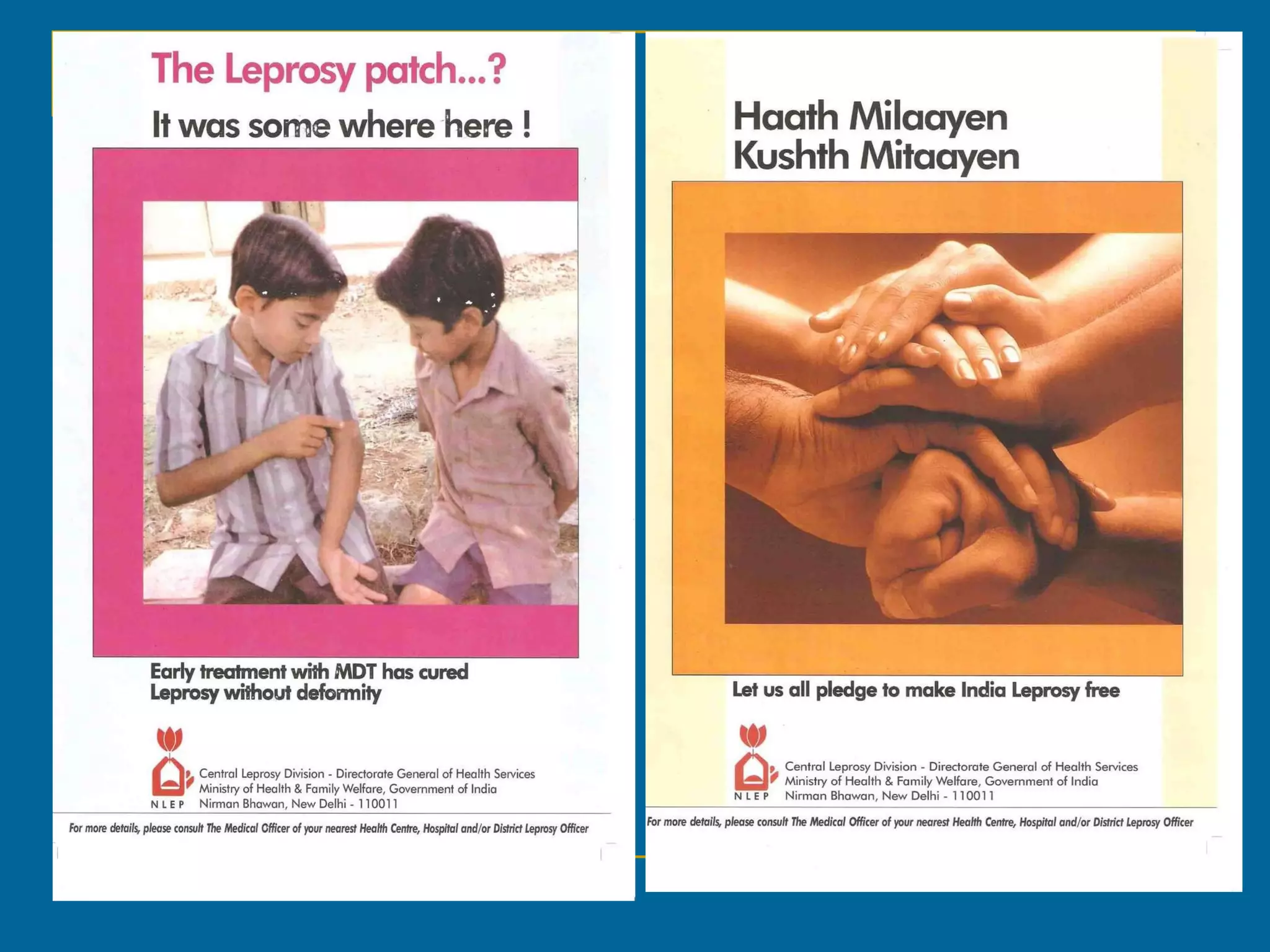
- In 1983, the goal shifted to eradication by 2000 with the National Leprosy Eradication Programme using multi-drug therapy and other strategies.
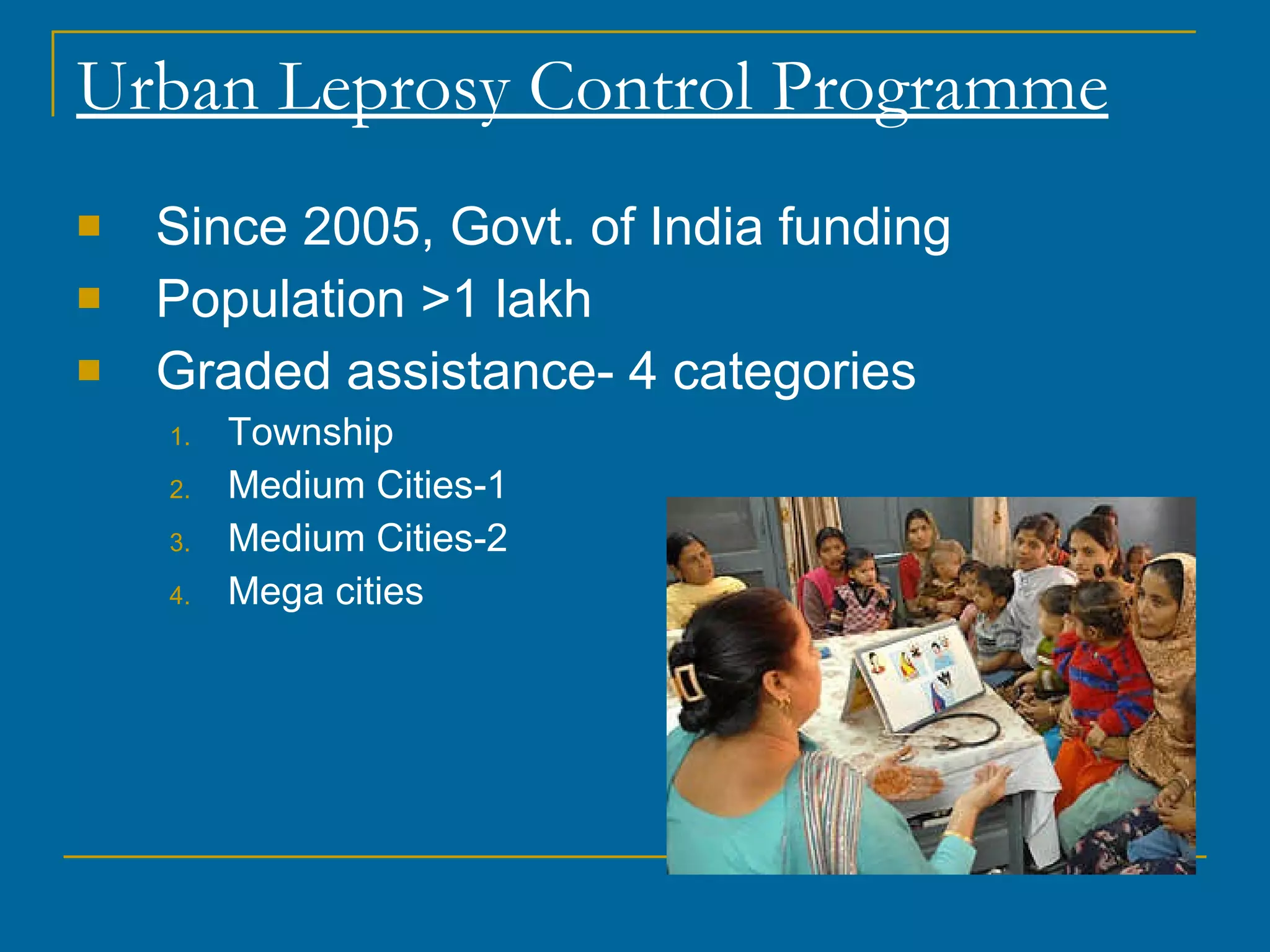
- Though prevalence was reduced, some states saw uneven progress, leading to the Modified Leprosy Elimination Campaign and other focused programs in the 2000s.
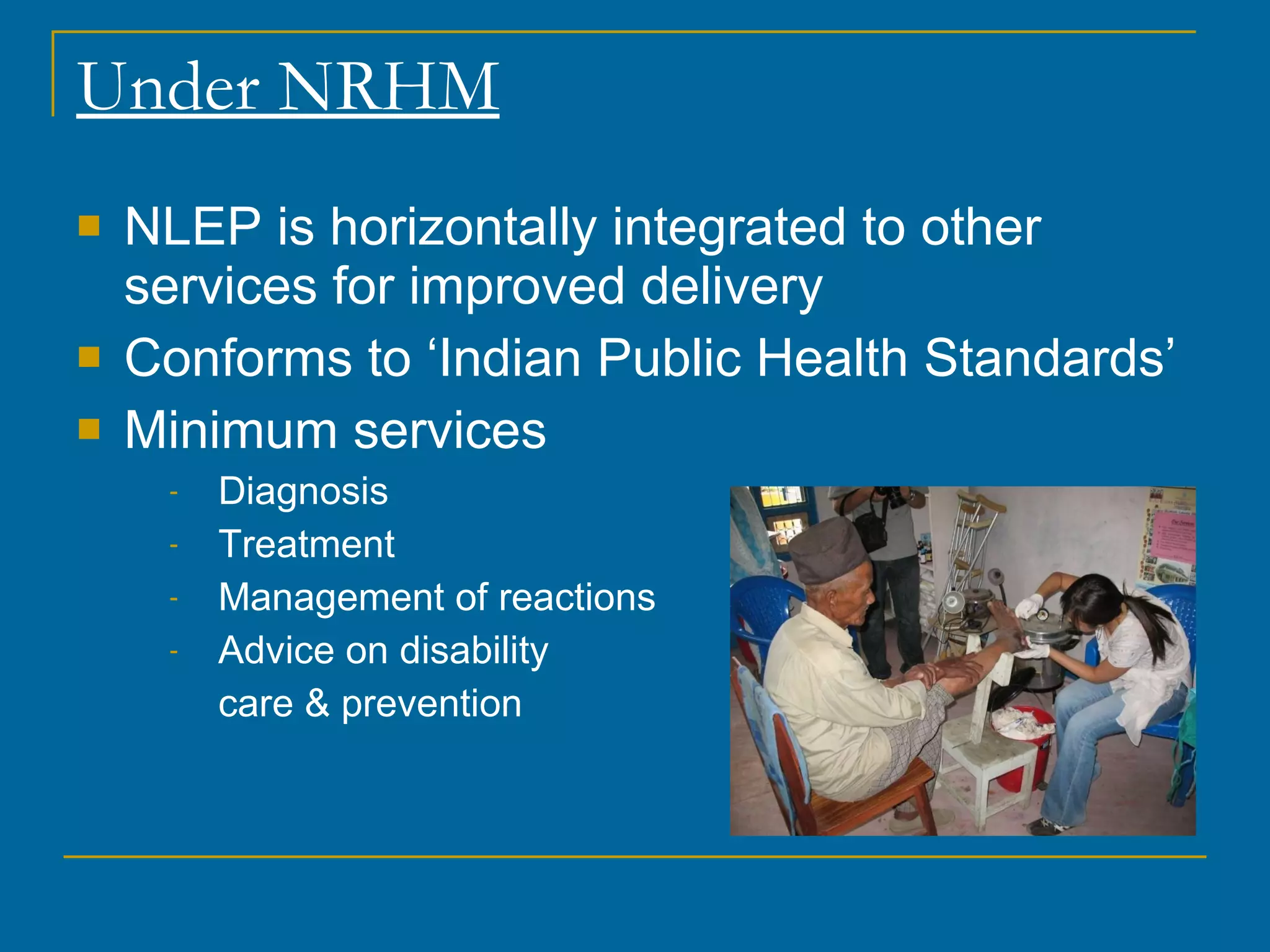
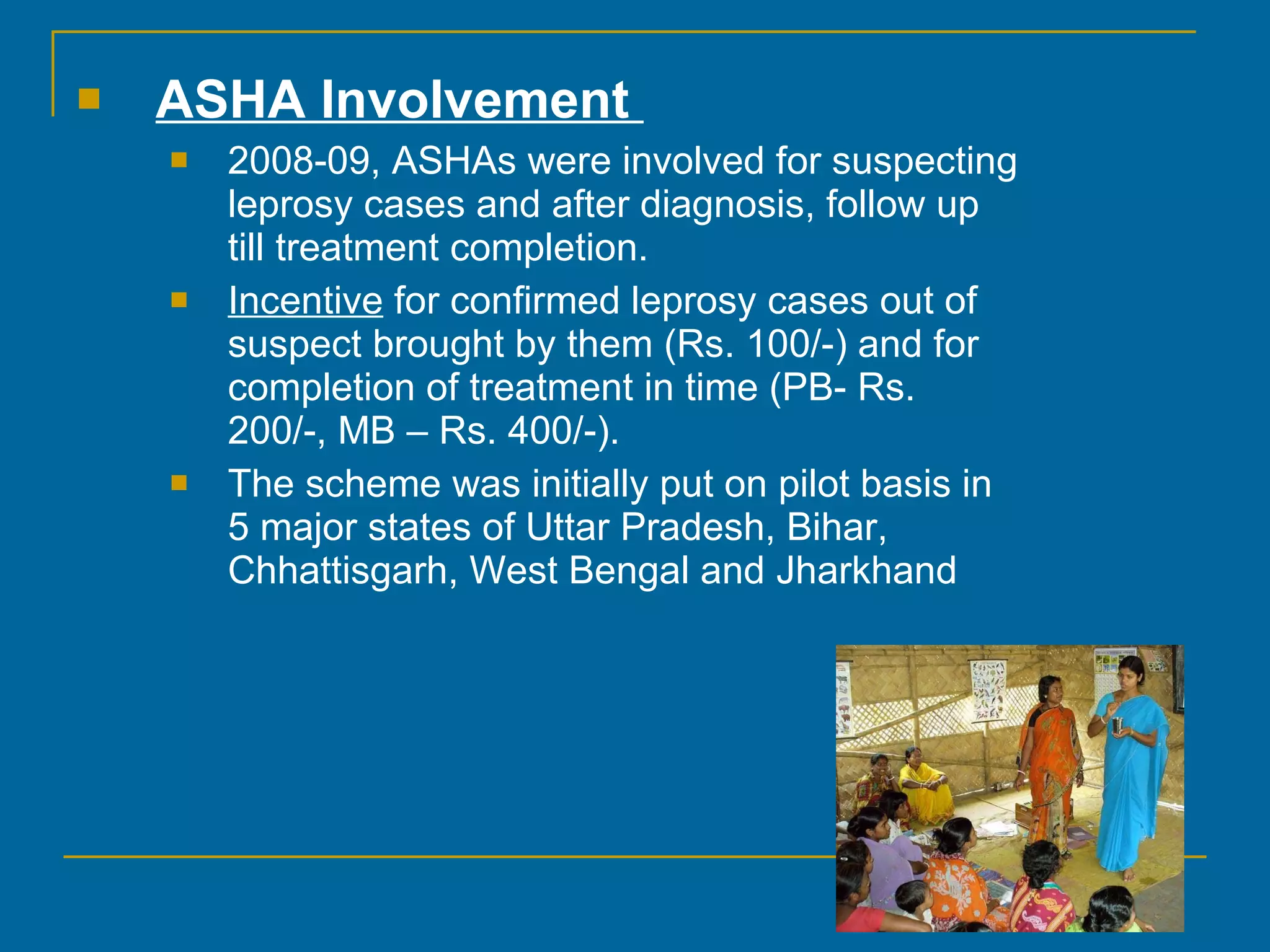
- Current strategies under NRHM integrate leprosy services and aim to maintain gains and eliminate leprosy at the district and block



























































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)



