The Universal Immunization Programme (UIP) was launched by the Government of India in 1985 to reduce mortality and morbidity from six vaccine preventable diseases (VPDs) and has evolved into a crucial part of the National Rural Health Mission since 2005. It provides routine immunizations, organizes campaigns, and addresses vaccine logistics while ensuring safety and efficiency through a cold chain system. Major achievements include the eradication of smallpox and a three-year polio-free status in India.



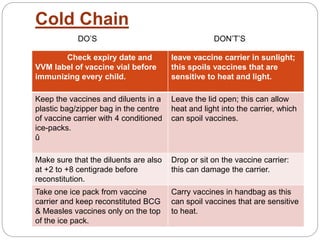
![ The diseases being targeted are diphtheria,
whooping cough, tetanus, poliomyelitis,
tuberculosis, measles and Hepatitis B. In addition
to these, vaccines for Japanese Encephalitis[2]
and Haemophilus influenzae type B are also
being provided in selected states.](https://image.slidesharecdn.com/universalimmunisationprogram-171120044520/85/Universal-immunisation-program-17-320.jpg)






















































![National programs dr jason [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/nationalprograms-drjasonautosaved-210917011725-thumbnail.jpg?width=640&height=640&fit=bounds)









![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)









