















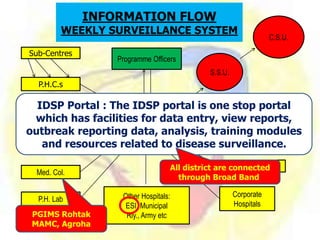












The Integrated Disease Surveillance Programme (IDSP) is a decentralized initiative launched in India to enhance disease monitoring and response to public health threats. It aims to consolidate data collection from various health sectors, improve response efficiency, and ensure timely actions for epidemic control and public health interventions. The program involves various stakeholders including government agencies, private sectors, and local communities to create a comprehensive approach for managing communicable diseases across the nation.









































































