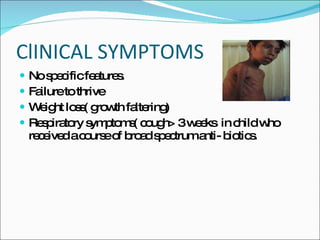
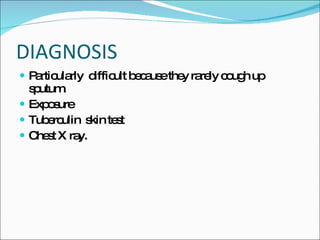
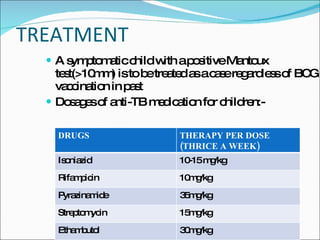
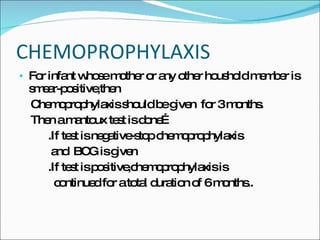
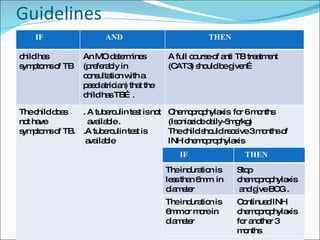
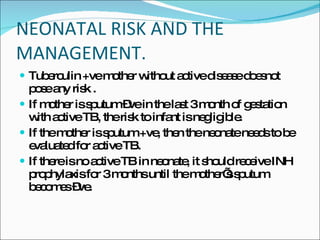
This document discusses tuberculosis (TB) in children, the relationship between TB and HIV, and TB during pregnancy. It notes that 10-20% of TB cases are in children under 5 years old. Children are usually sputum-negative and not infectious. The main sources of infection are adults with sputum-positive TB. Treatment involves several anti-TB drugs given in specific doses over several months. Chemoprophylaxis is recommended for children exposed to sputum-positive individuals. Co-infection with HIV greatly increases the risk of active TB. Diagnosis is more difficult and extra-pulmonary TB is more common. Standard TB treatment is still used but drug interactions with HIV medications must be considered. TB in pregnancy does not typically















![16007107 ade-of-anti tubercular-drugs-mdr-tb[1]](https://cdn.slidesharecdn.com/ss_thumbnails/16007107-ade-of-antitubercular-drugs-mdr-tb1-100825234809-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)





















































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)















