Downloaded 237 times






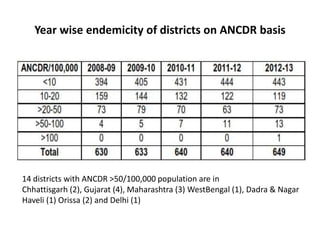


This document provides an overview of leprosy in India, including its transmission, diagnosis, treatment, and the national program to eliminate leprosy. Some key points: - Leprosy primarily affects the skin, nerves, and mucous membranes and can cause deformities. It is spread through droplets and untreated patients are the main reservoir. Multi-drug therapy can cure patients and interrupt transmission. - India's National Leprosy Elimination Program aims to integrate services, provide MDT, conduct surveillance, increase awareness, and prevent disabilities. Through these strategies, the national prevalence rate has declined and most states have achieved elimination targets. - However, some areas still have high rates and ongoing efforts include training









































































































