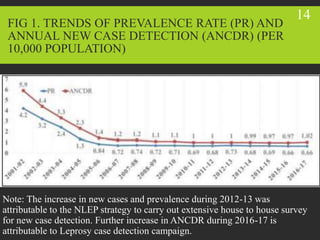
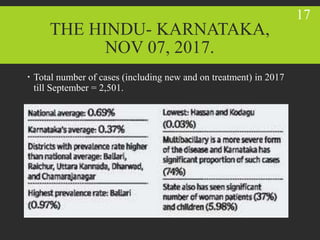
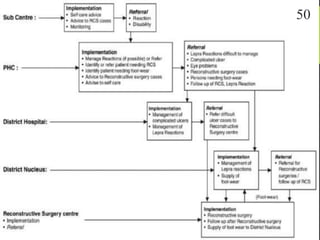
The National Leprosy Eradication Programme (NLEP) in India aims to eliminate leprosy, prevent disabilities, and reduce stigma associated with the disease. Key components of the program include case detection and treatment, disability prevention and rehabilitation, information/education campaigns, and human resource training. The NLEP is decentralized and integrated into general healthcare. It focuses on early detection and treatment using multidrug therapy, as well as preventing disabilities through services like reconstructive surgery. Monitoring and evaluation involves routine reporting and field visits to track indicators like prevalence and detection rates.