Download as PDF, PPTX




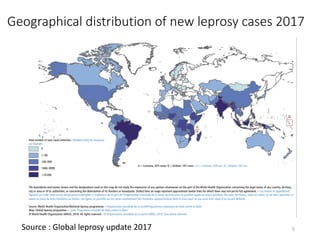















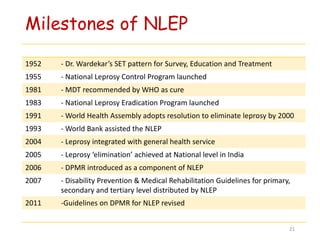






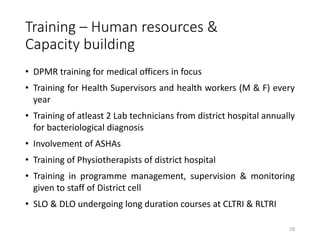














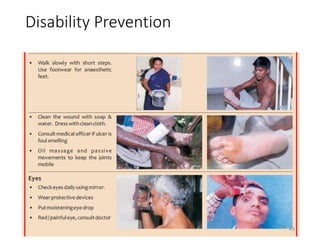

































The document presents an overview of the National Leprosy Eradication Program in India, highlighting the epidemiological status, program objectives, strategies for leprosy case detection, and disability prevention efforts. It provides data on leprosy prevalence and new case detection rates, outlines training and human resource development, and discusses funding and support from various agencies. The presentation emphasizes the importance of community awareness campaigns and ongoing monitoring and evaluation to combat leprosy effectively.



































































