Downloaded 63 times

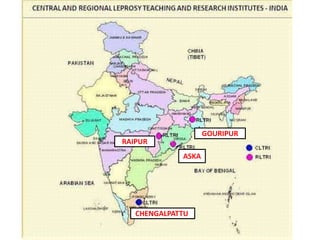



The National Leprosy Eradication Program in India has achieved major milestones since its inception in 1955. Through strategies like introducing multi-drug therapy in 1983 and nationwide campaigns, prevalence rates have declined from over 20 per 10,000 people in the early 1990s to less than 1 per 10,000 in 2005, allowing India to achieve the goal of eliminating leprosy at the national level. Ongoing challenges include preventing disability through early detection, reducing stigma, ensuring treatment adherence, and sustaining control efforts. International support from organizations like WHO and NGOs continues to aid India's leprosy elimination efforts through technical guidance and resource provision.









































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

