Downloaded 400 times
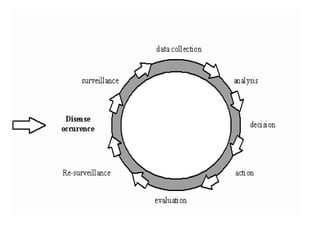
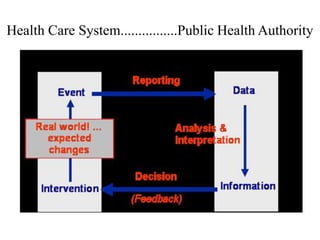
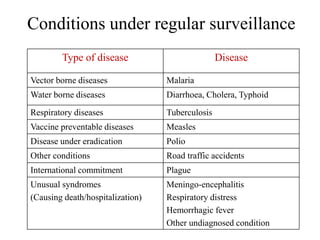
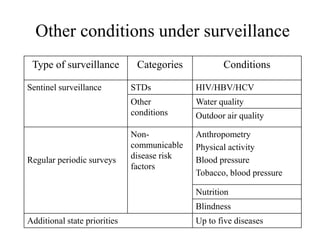
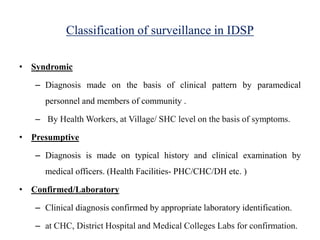
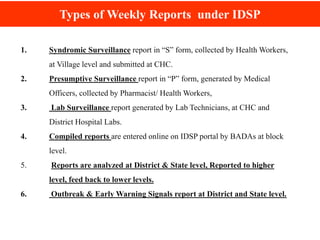
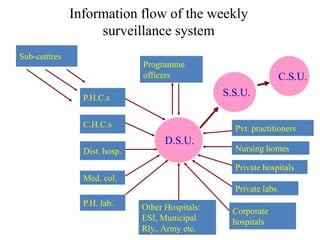
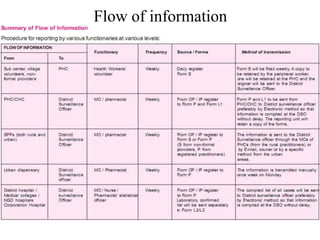
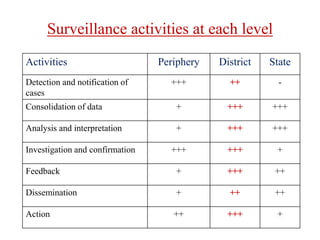
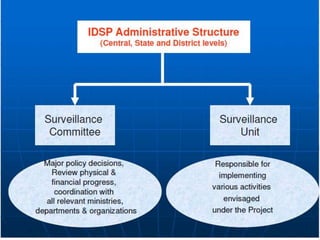
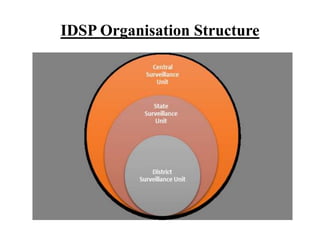
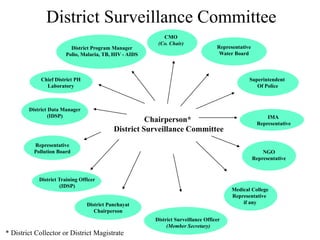

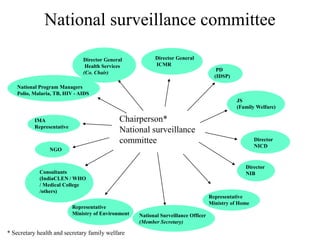
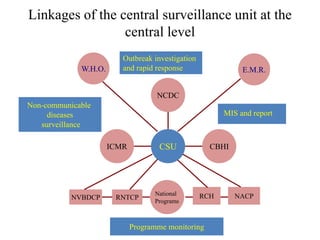
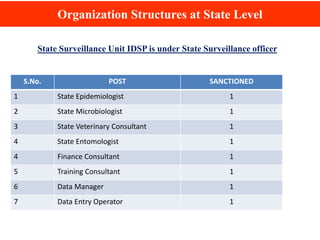
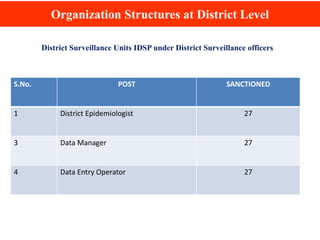
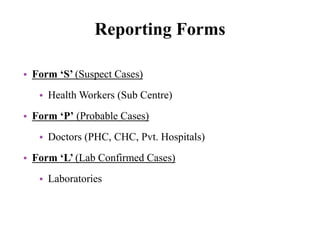
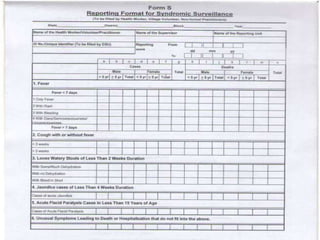
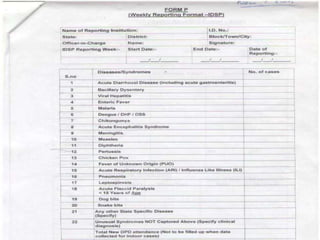
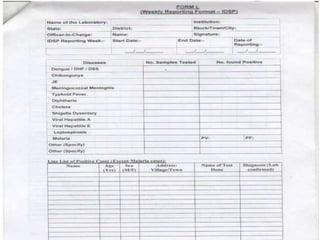
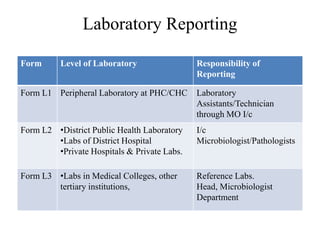
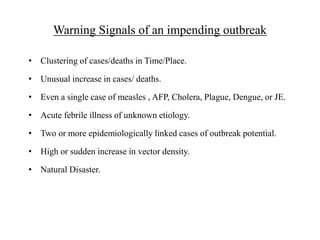
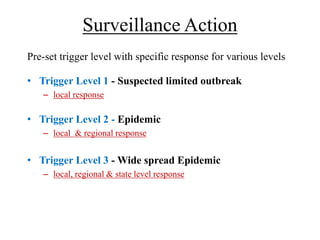

The document provides information about the Integrated Disease Surveillance Programme (IDSP) in India. It discusses that IDSP aims to establish a decentralized disease surveillance system to detect early warning signals of outbreaks. Key elements of IDSP include detection and reporting of health events, investigation and confirmation of cases, collection and analysis of surveillance data, and feedback to initiate public health responses. IDSP implementation is organized at the national, state, and district levels with defined roles and reporting structures. The program coordinates surveillance of both communicable and non-communicable diseases using standardized reporting forms.





















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
















