P
4
3
2
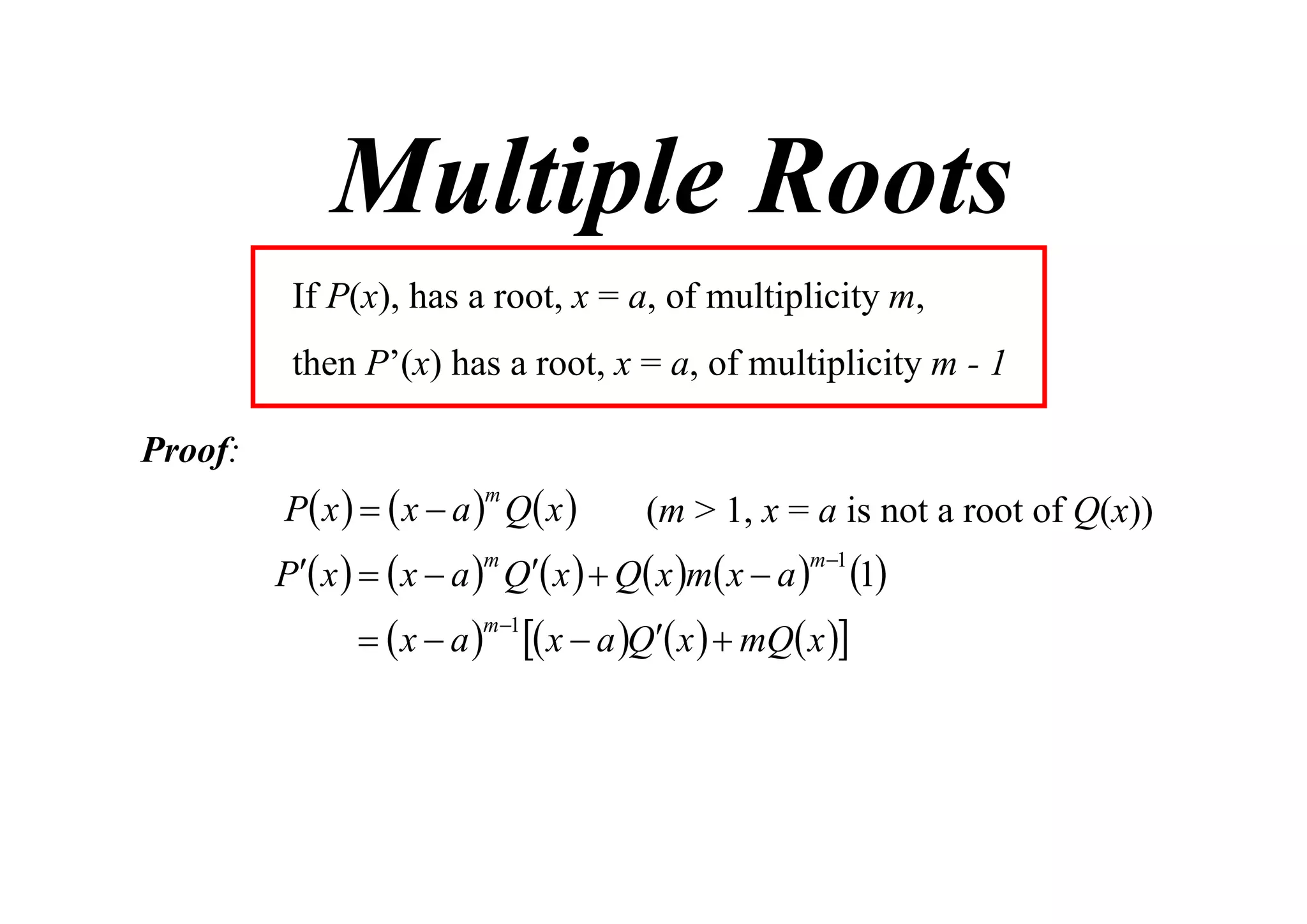
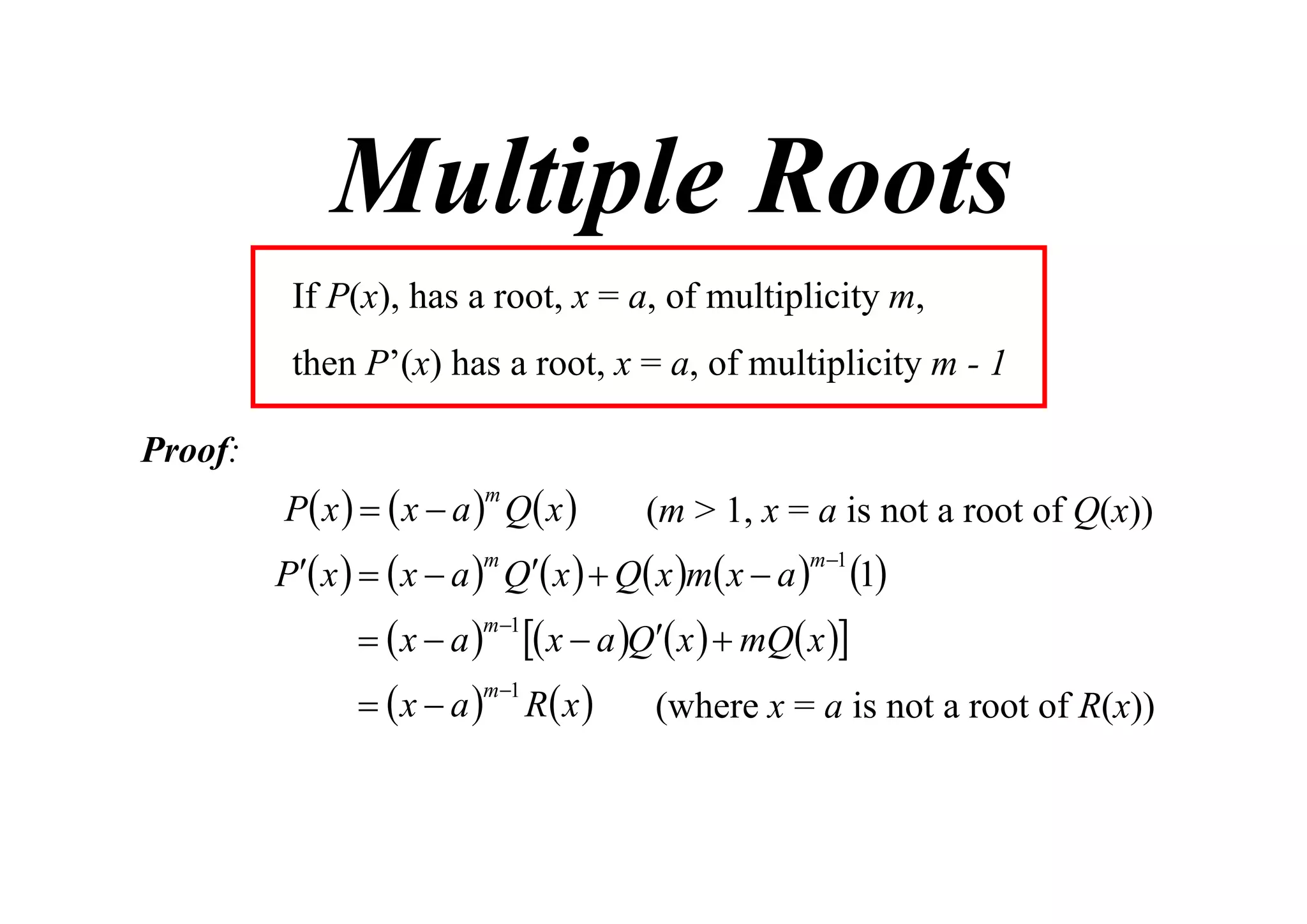
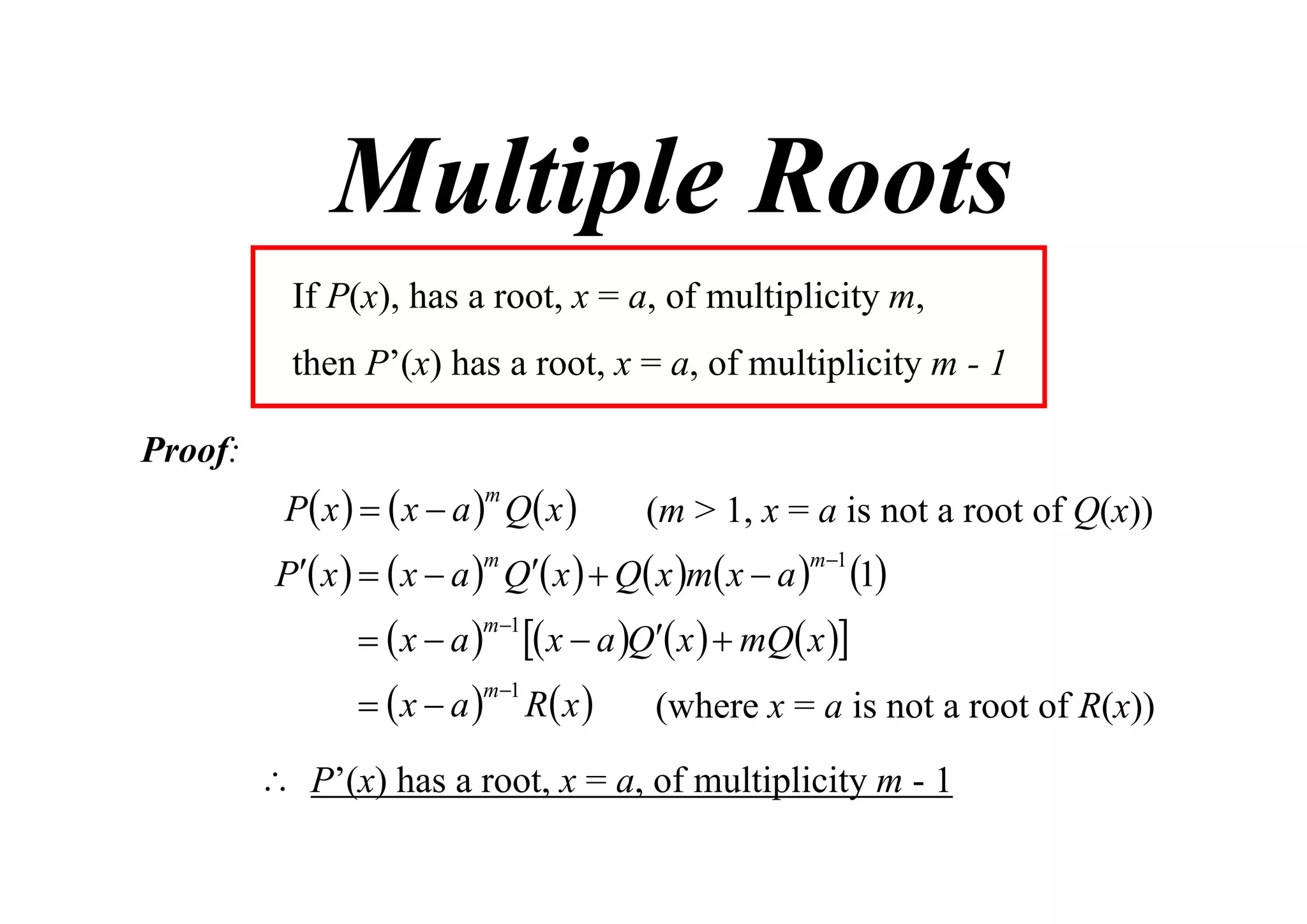
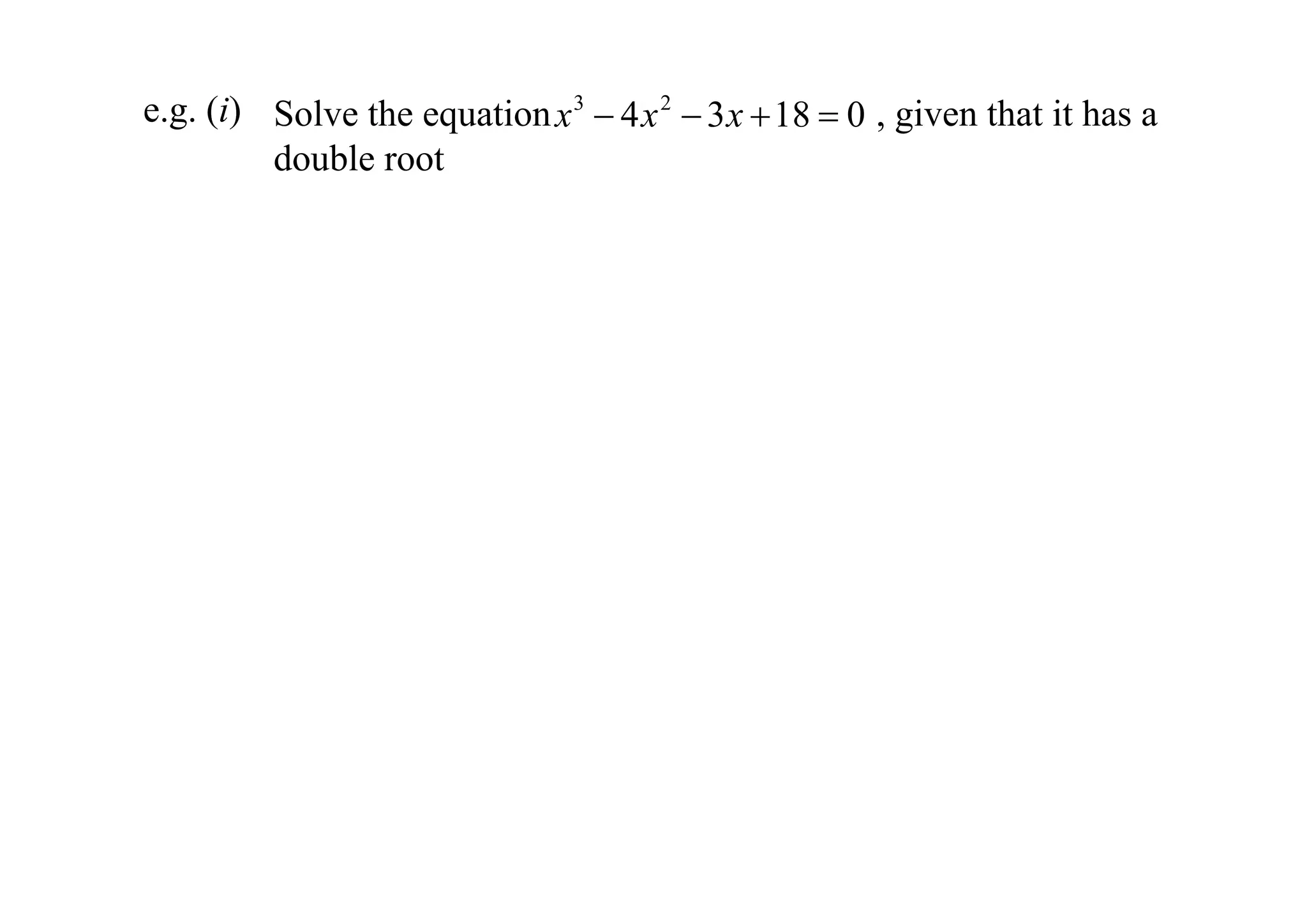
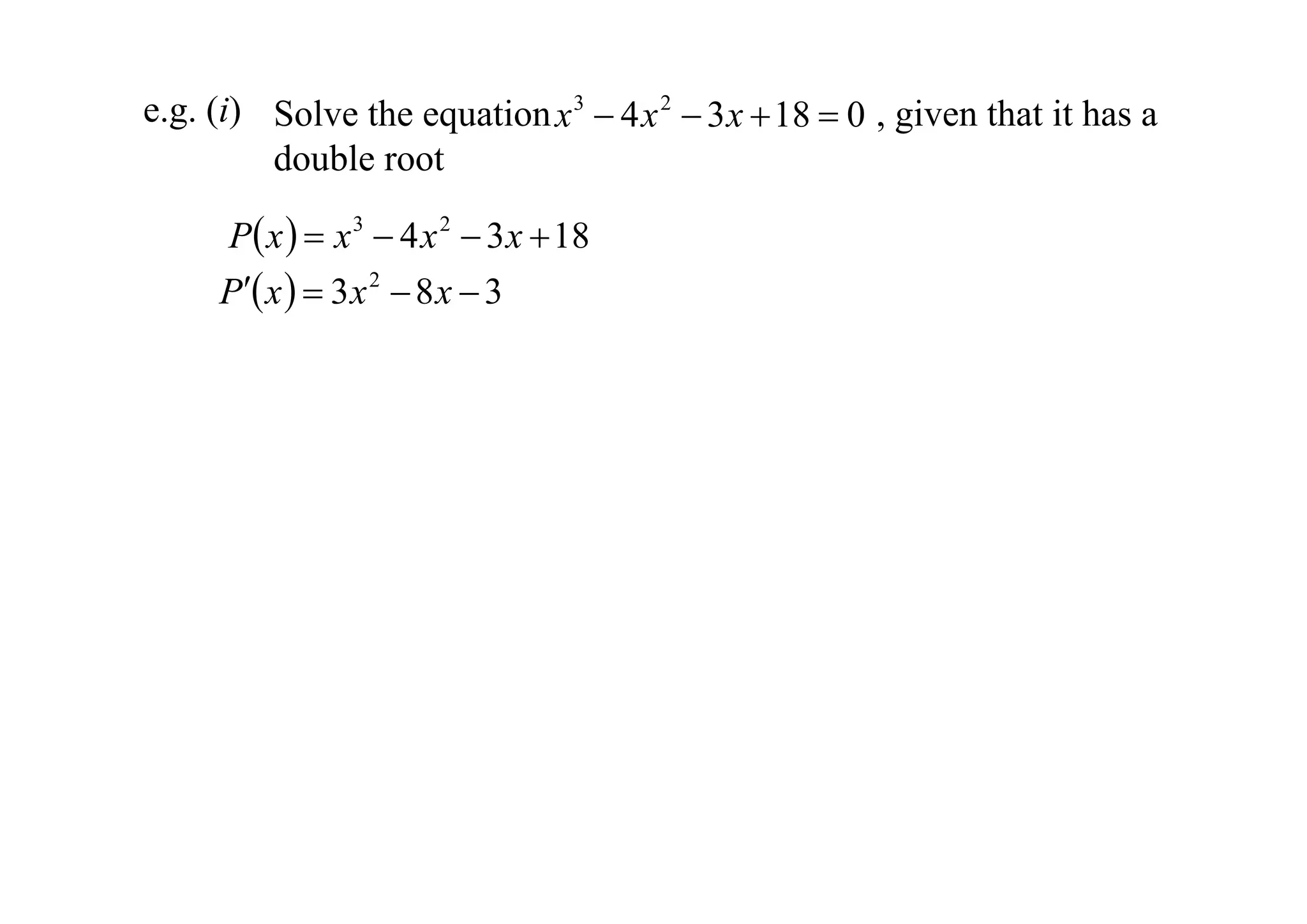
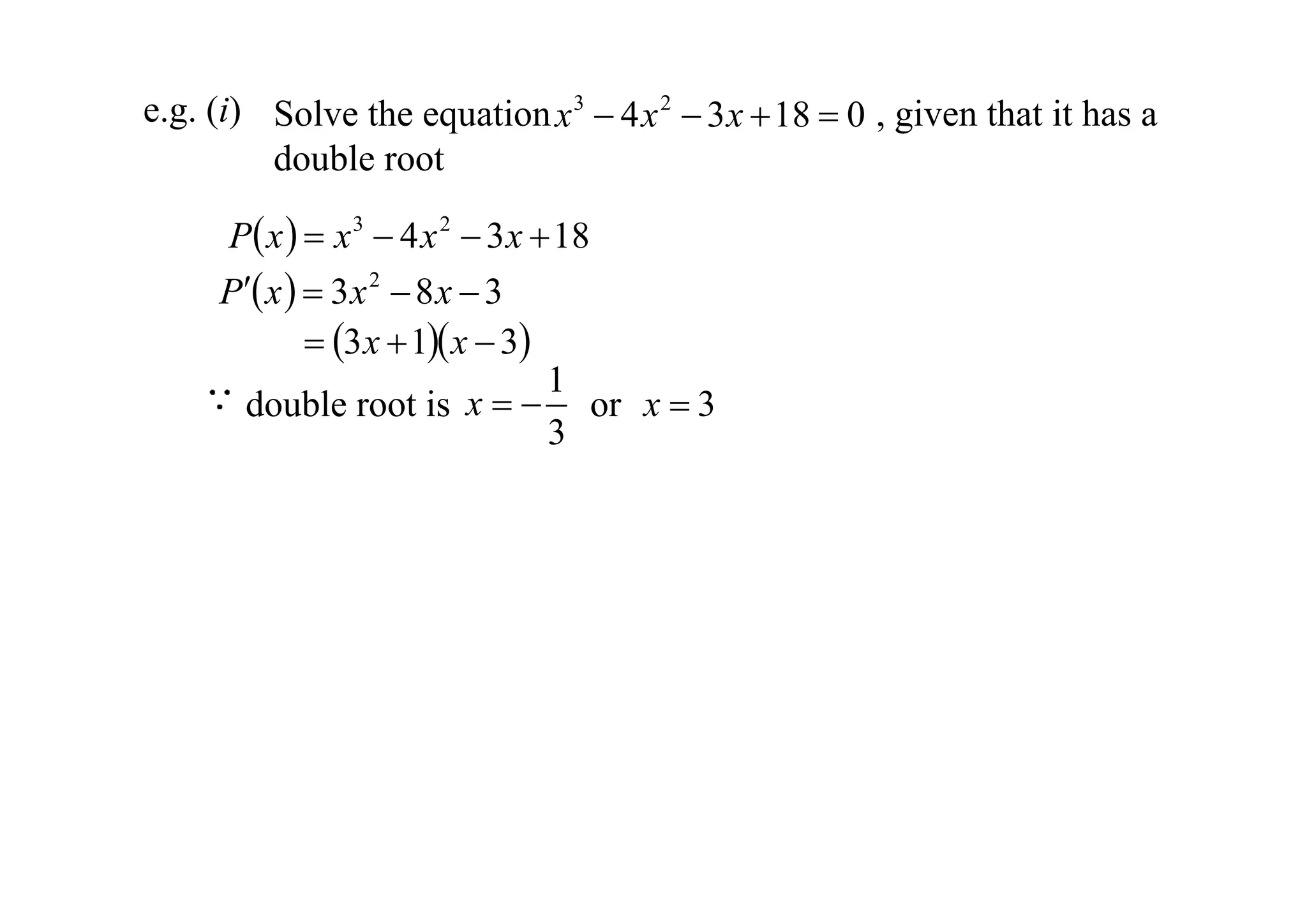
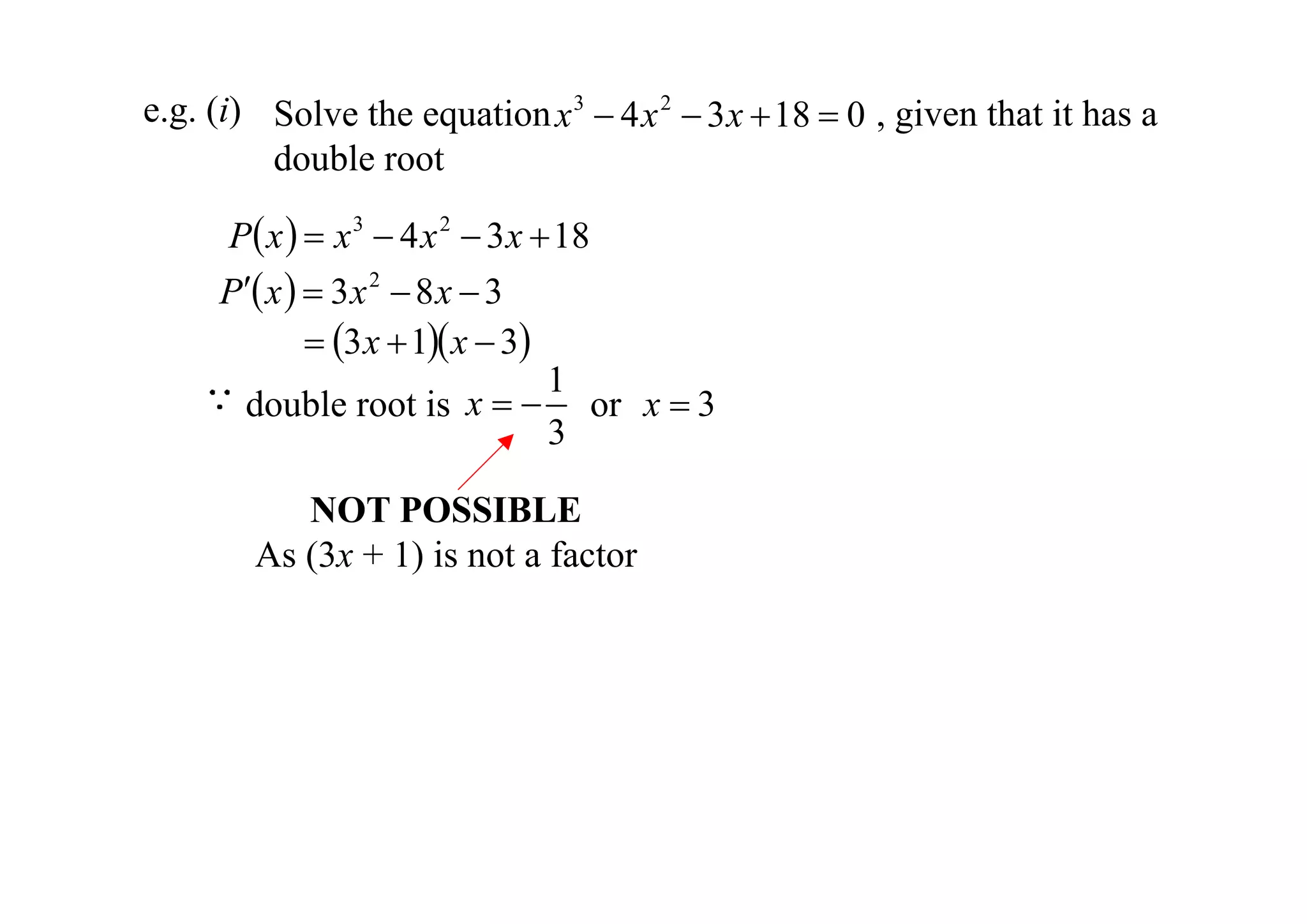
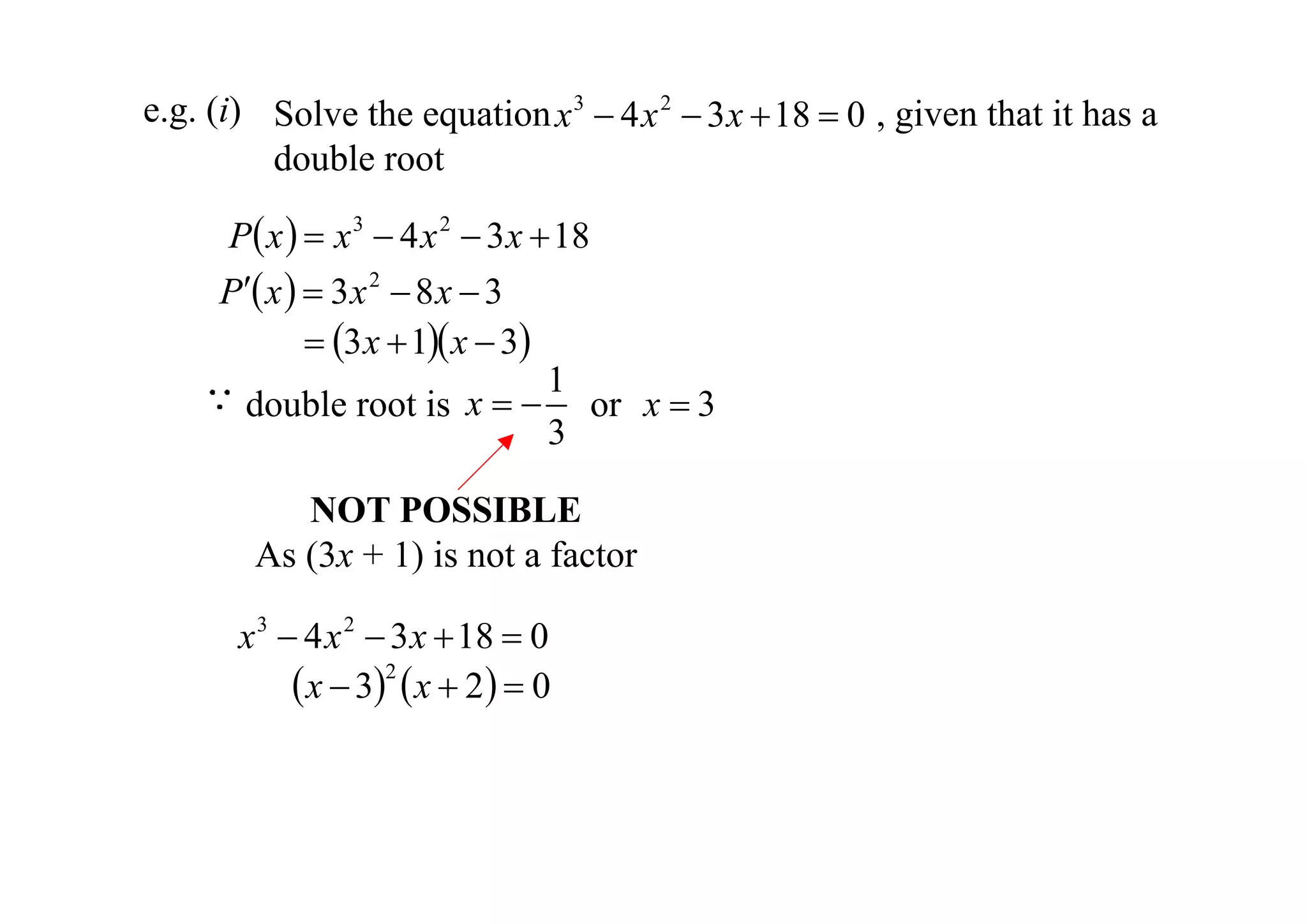
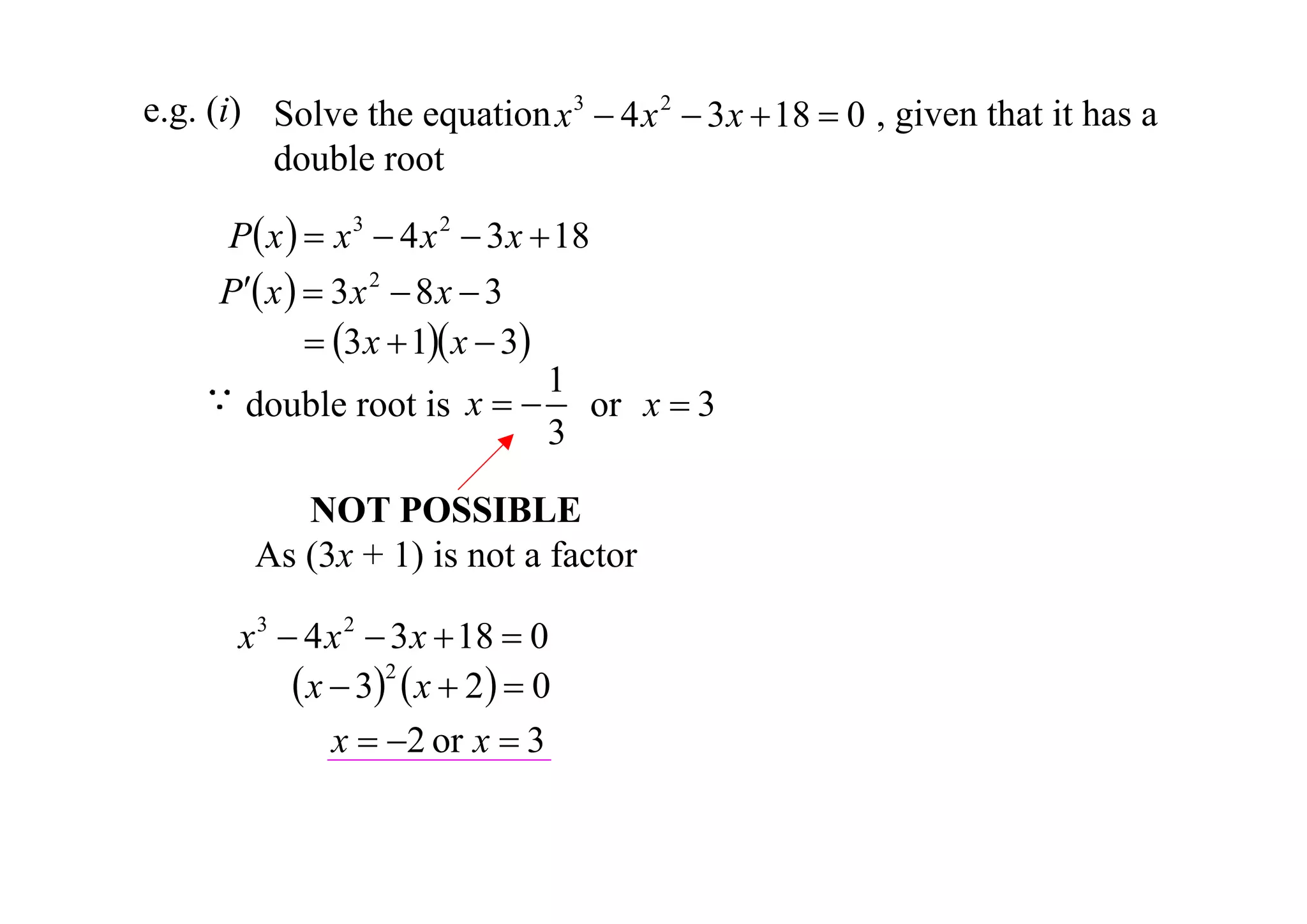
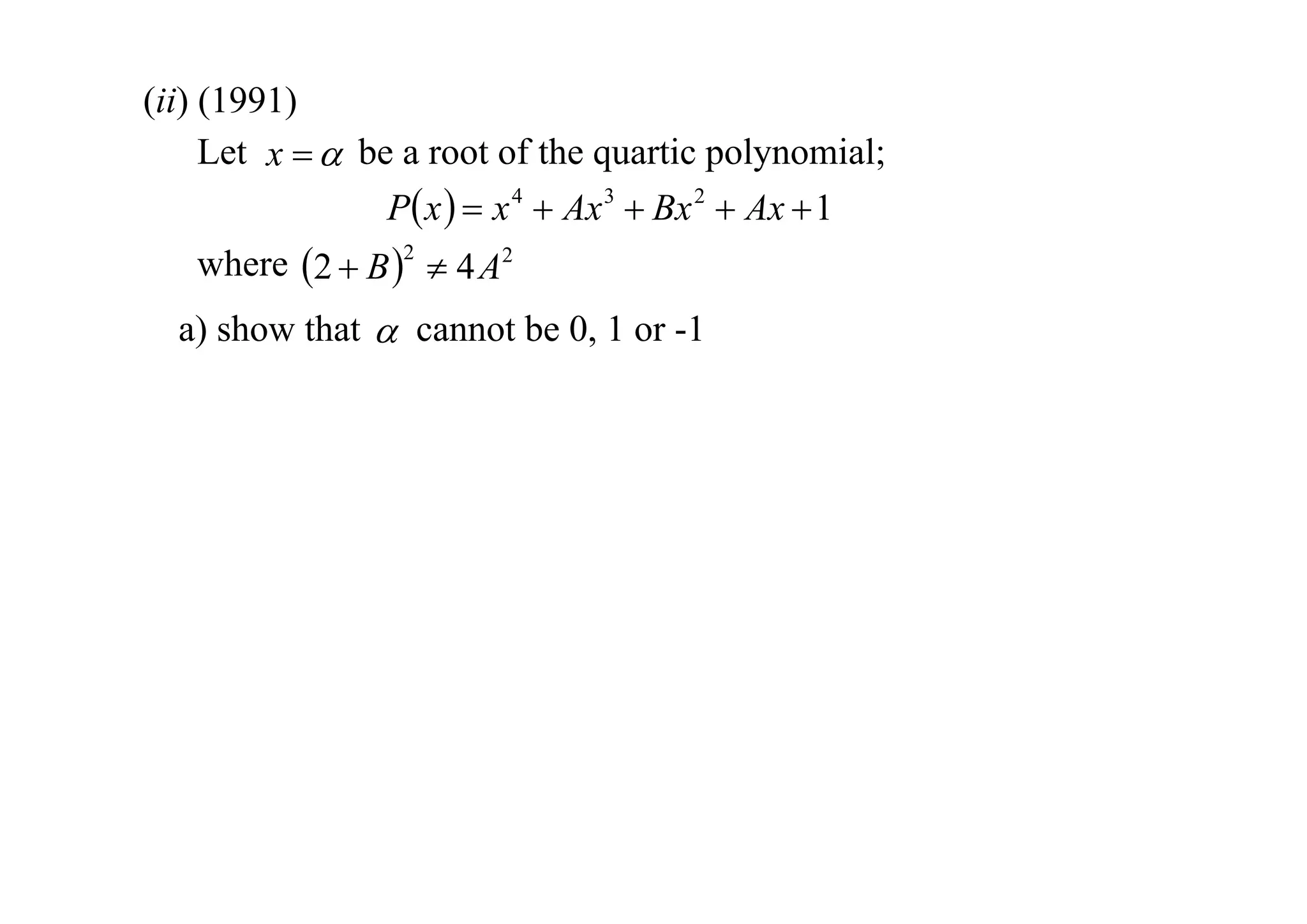
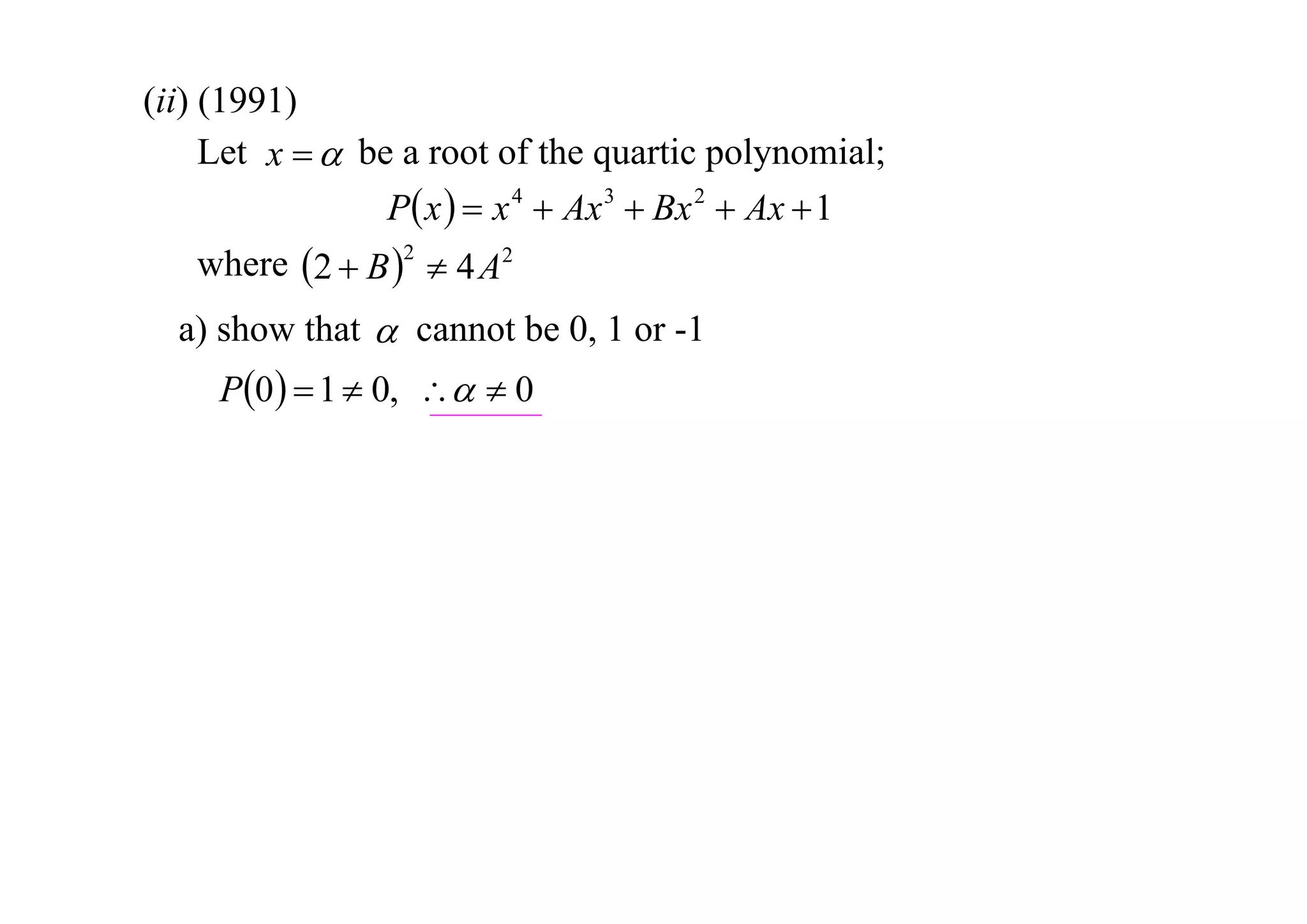
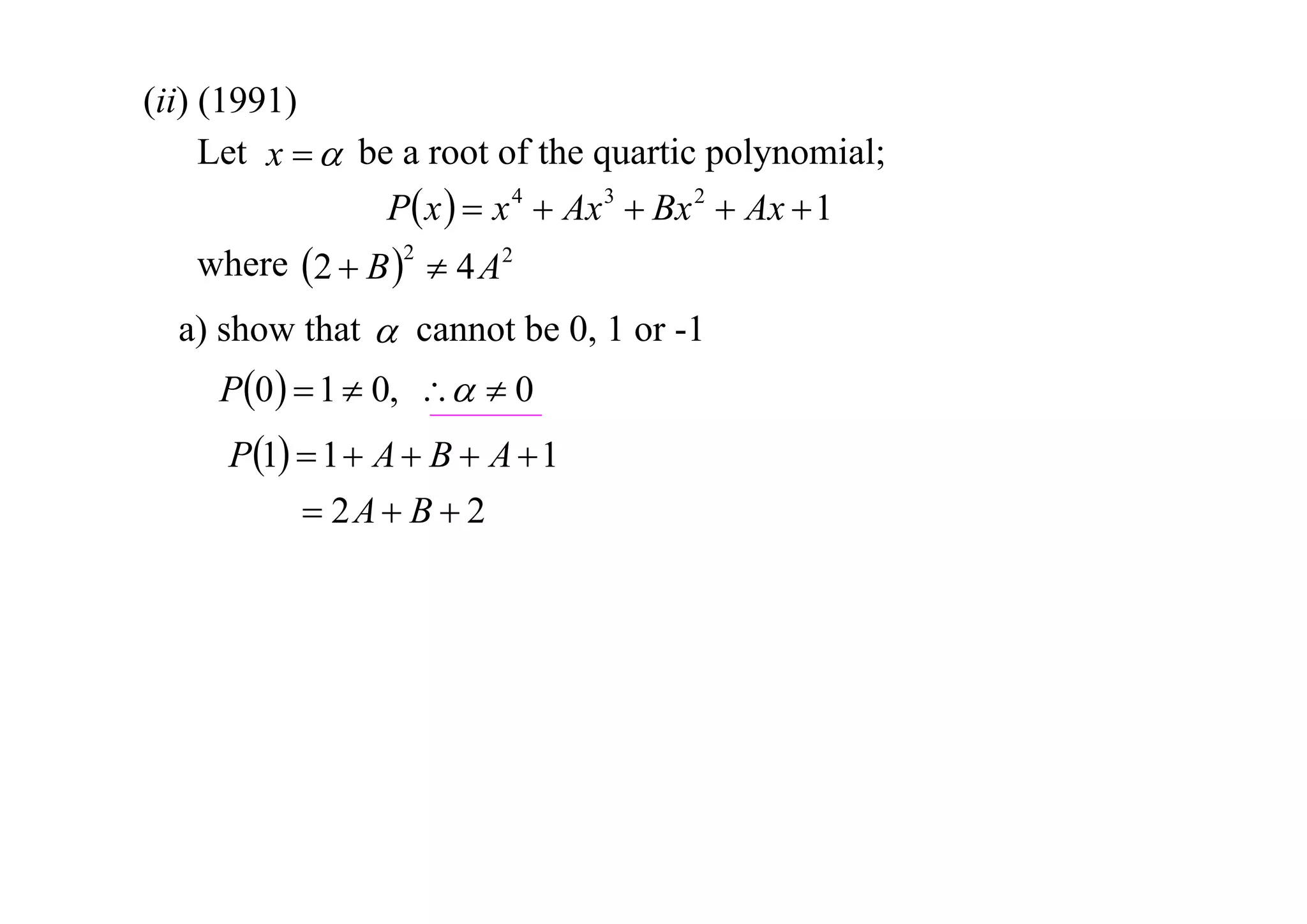
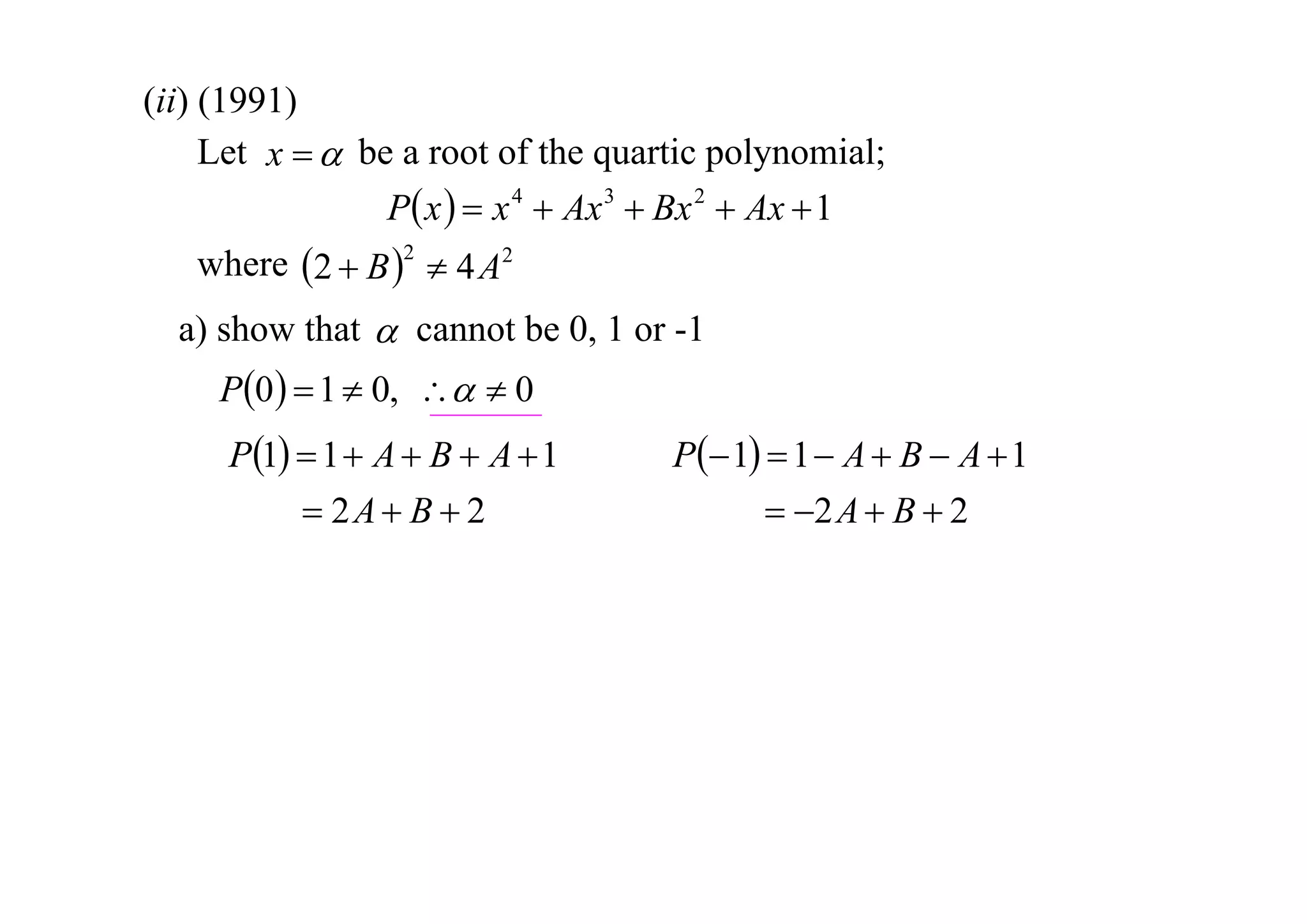
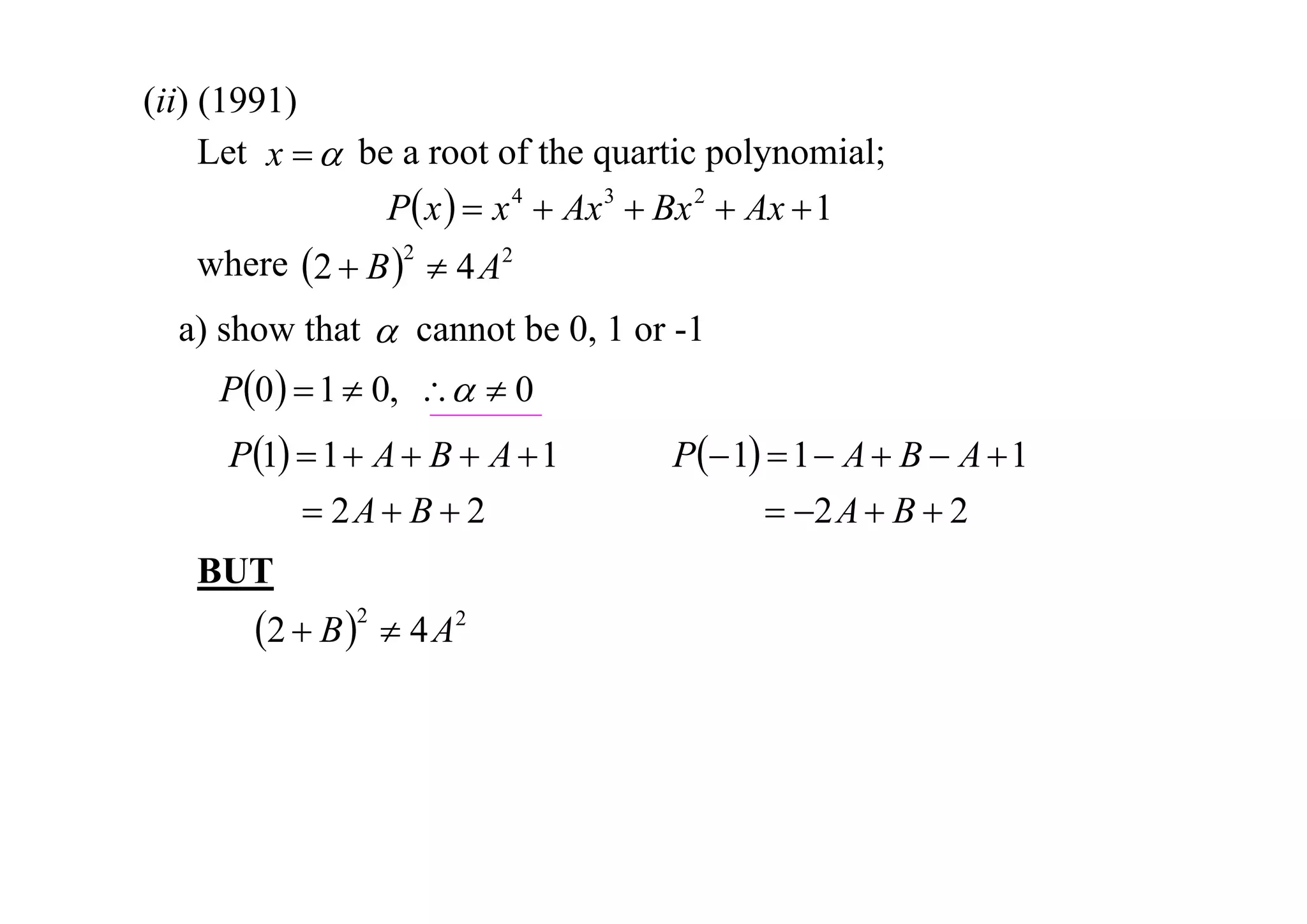
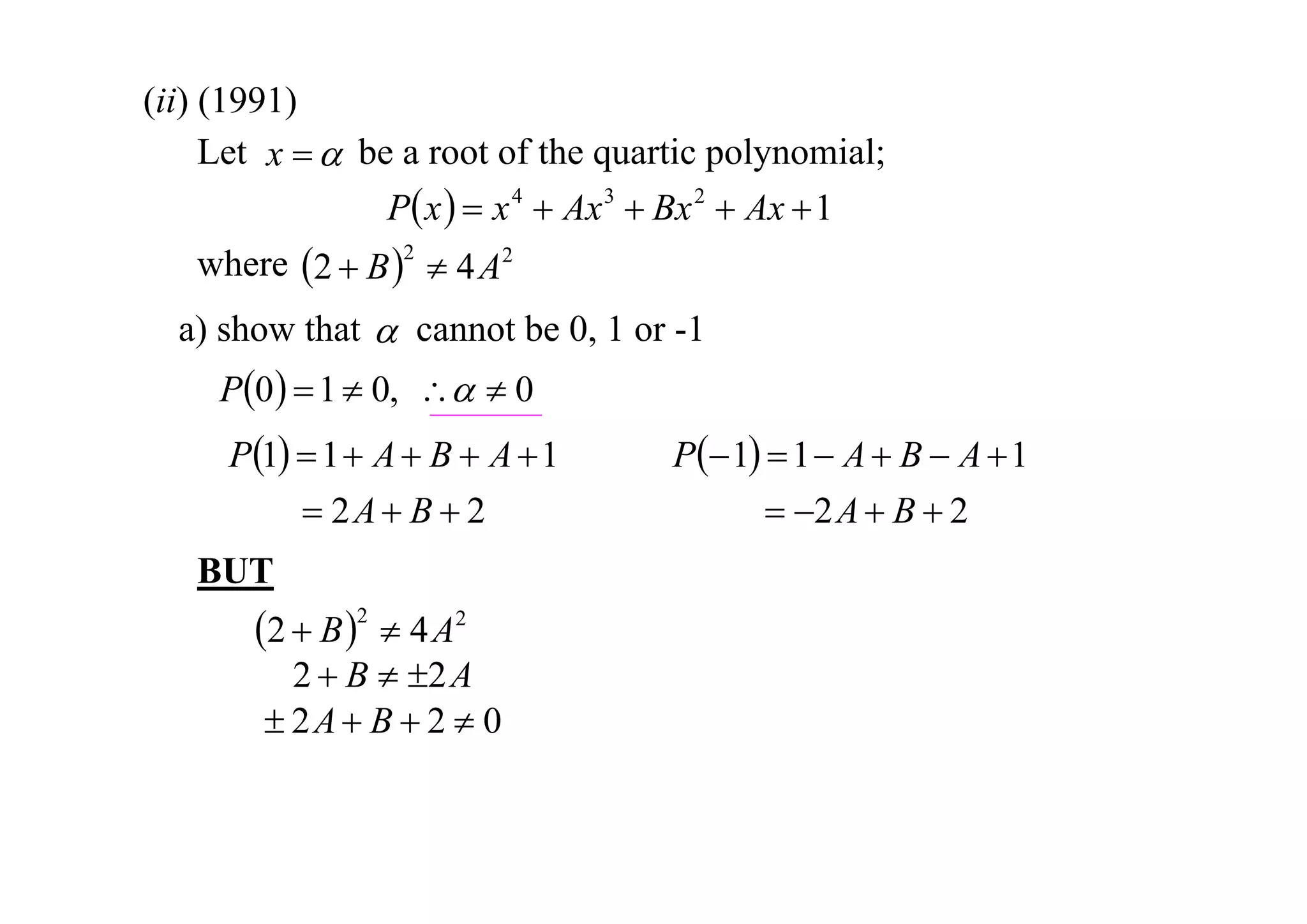
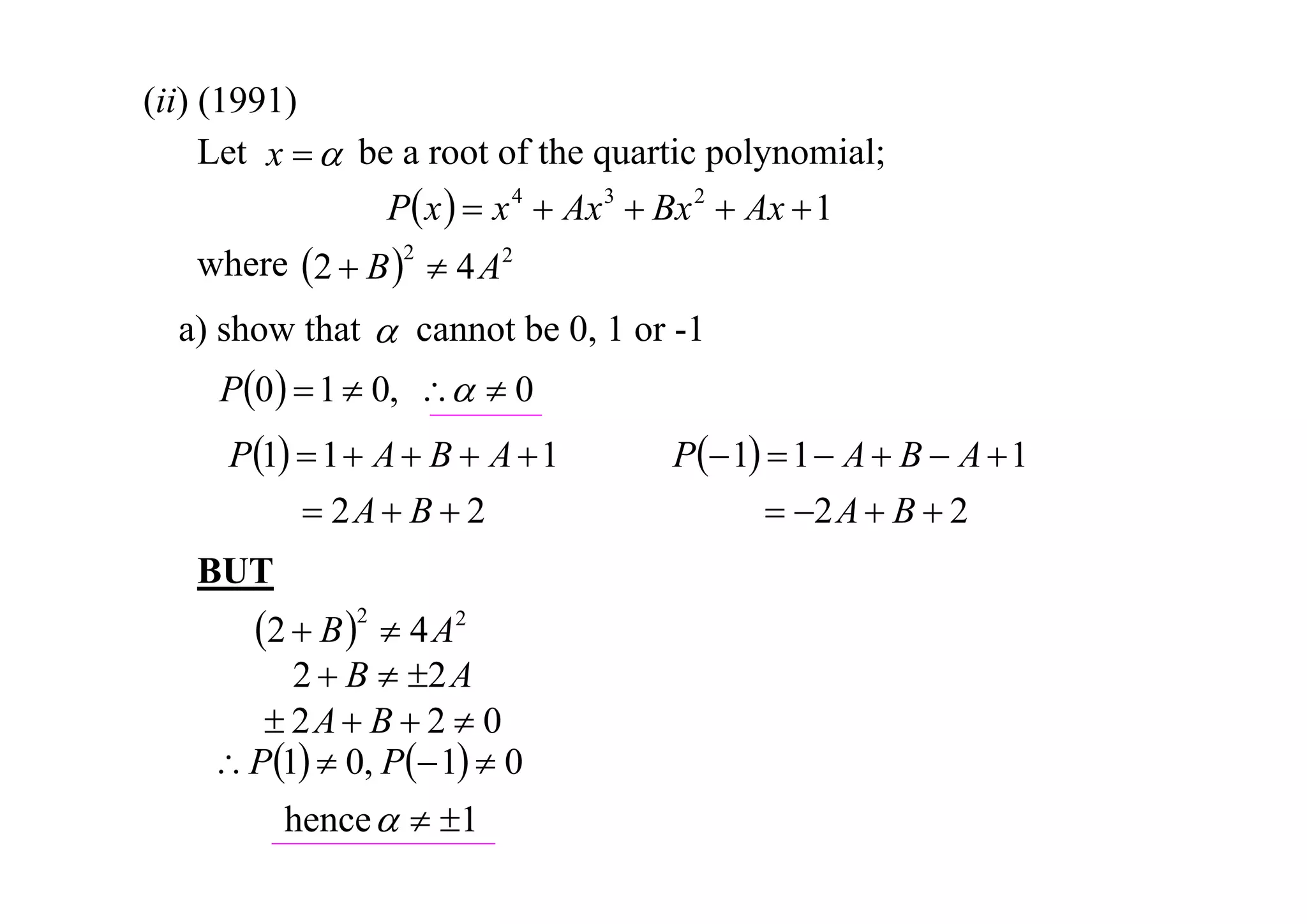
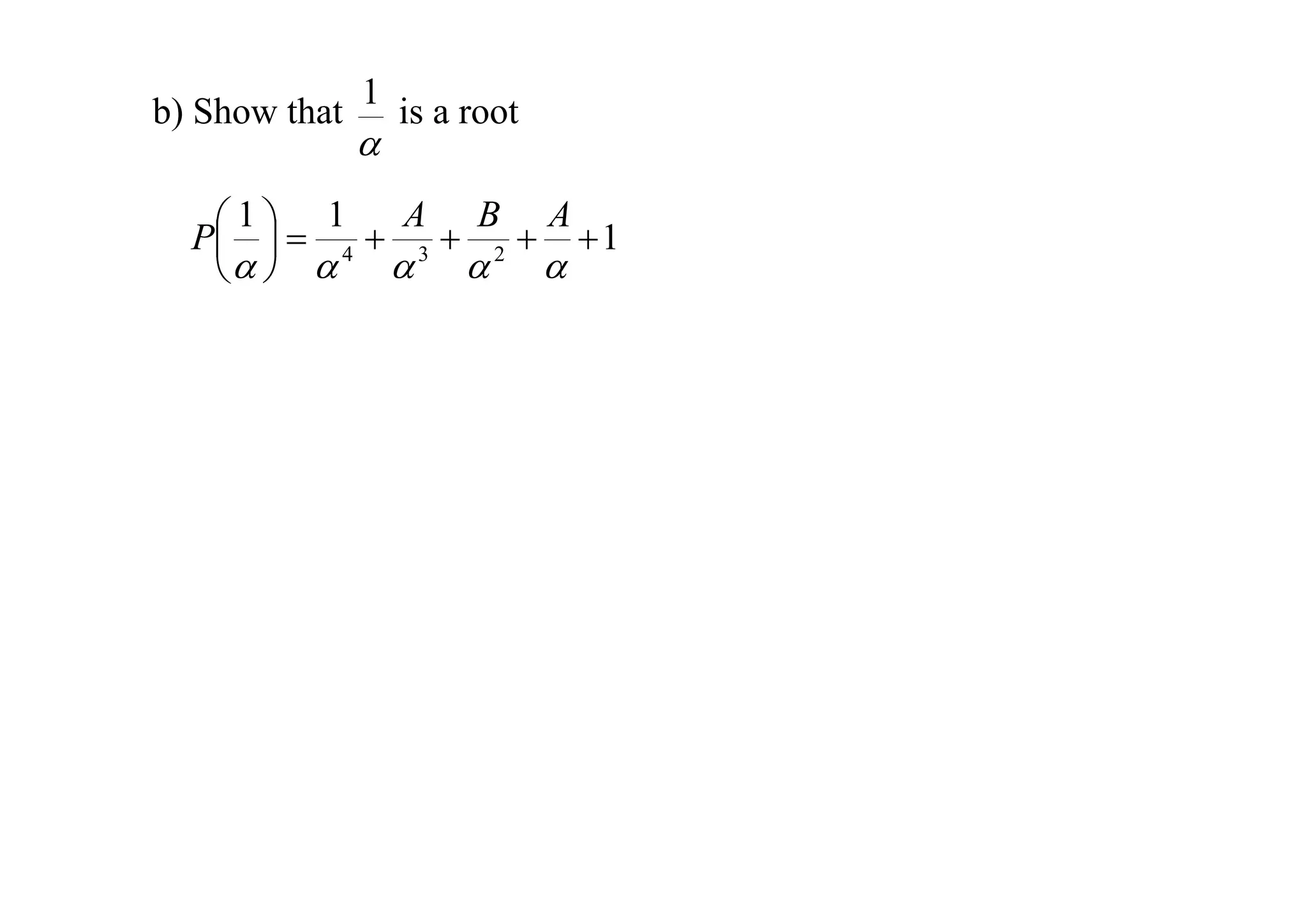
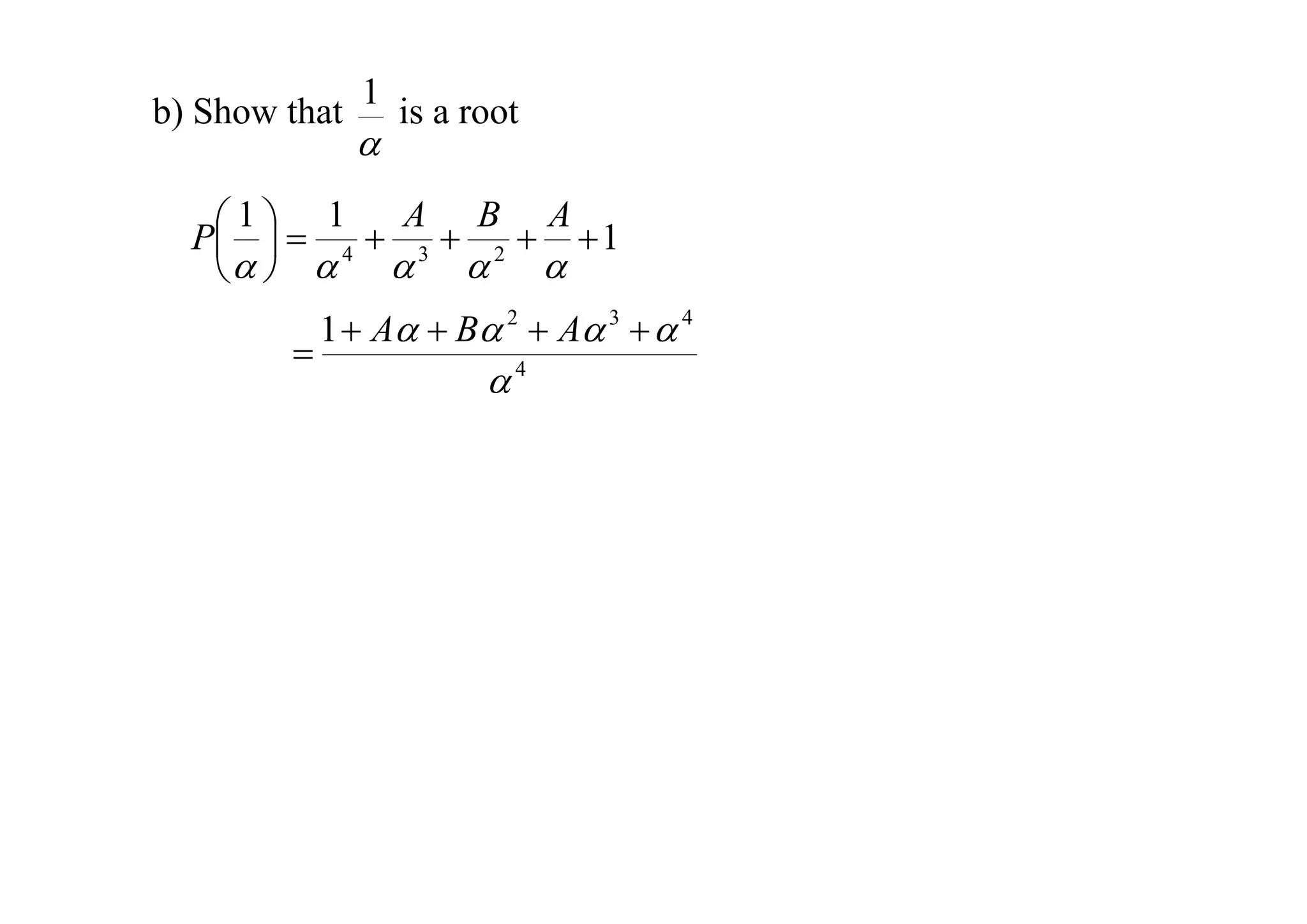
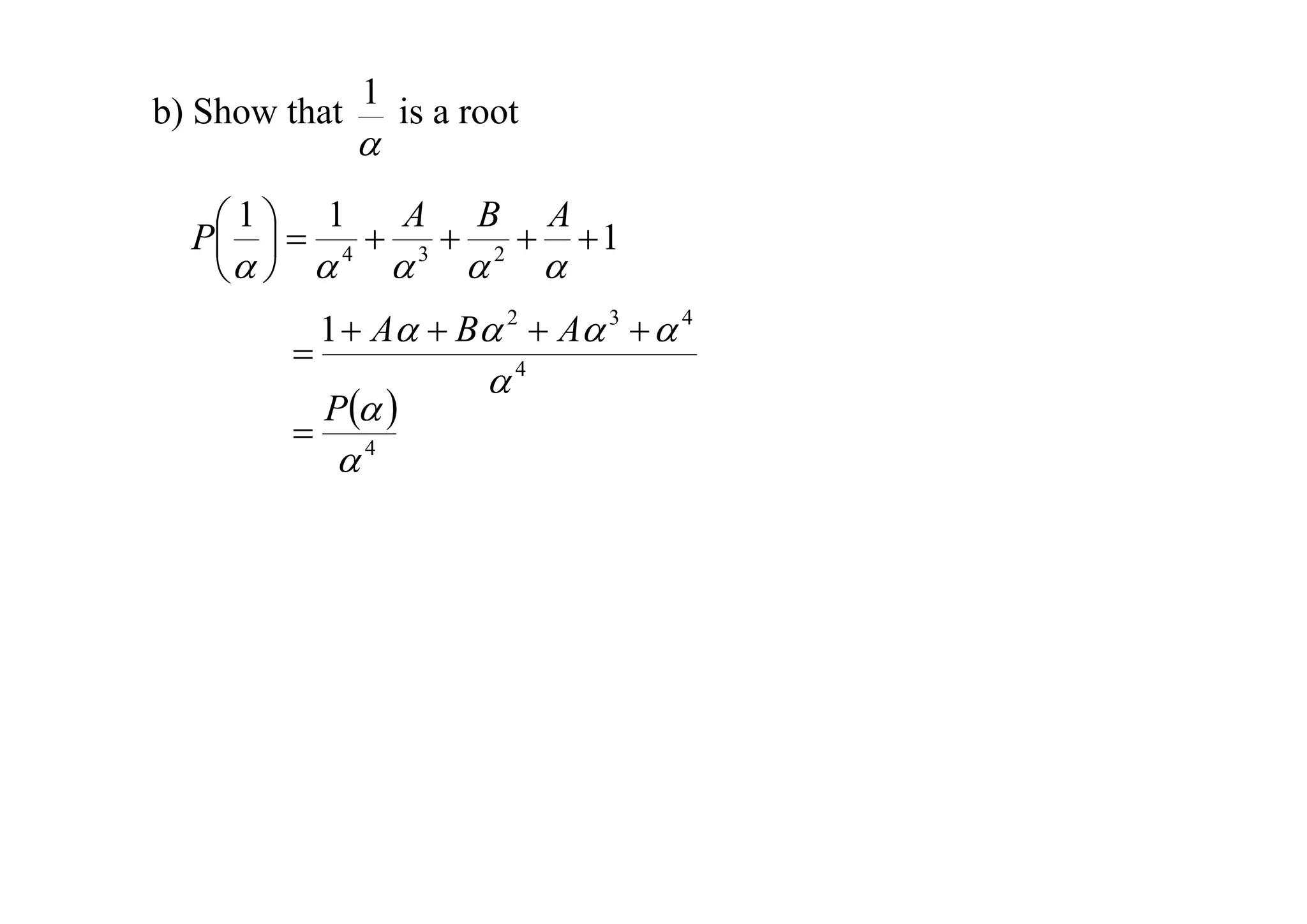
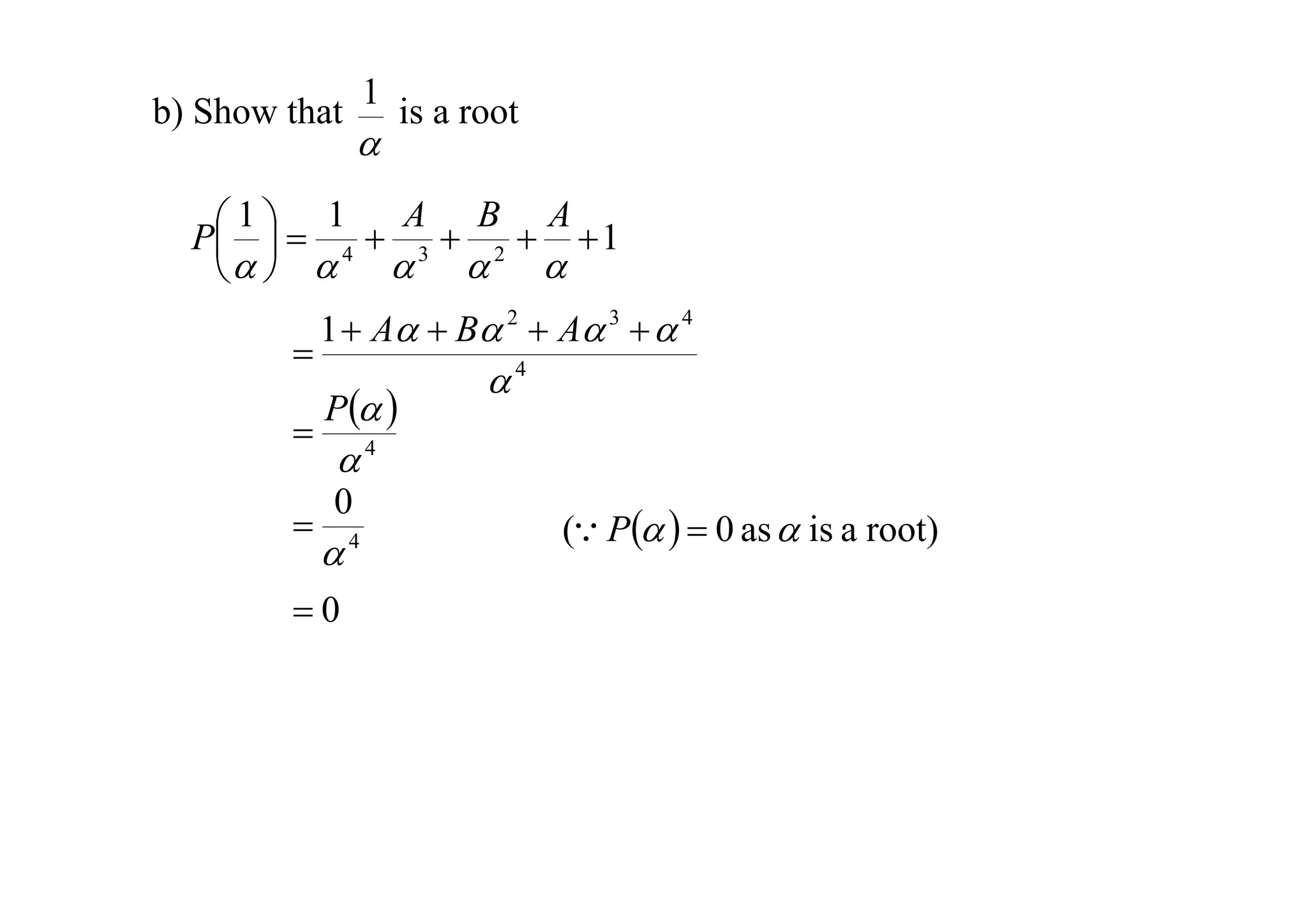
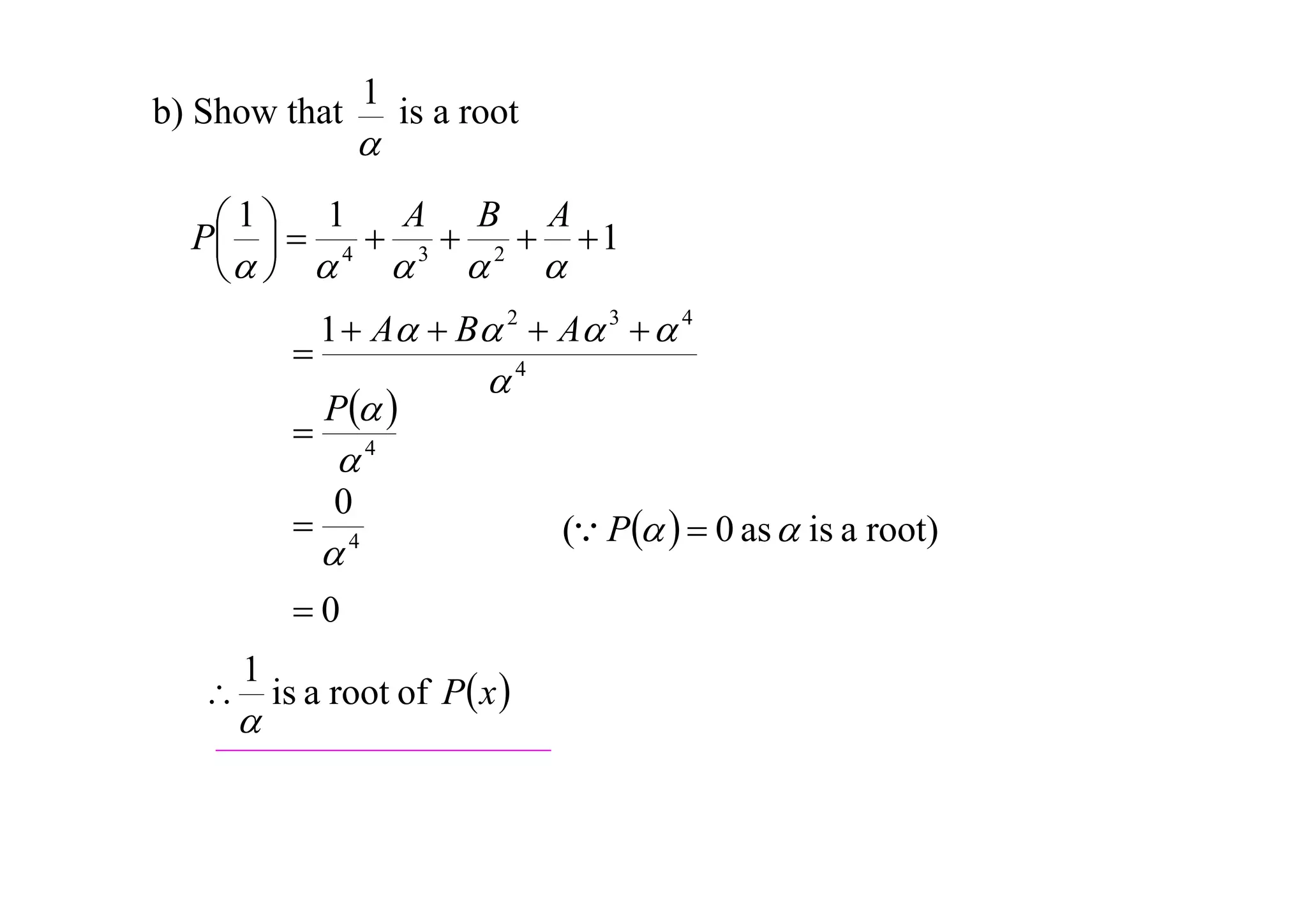
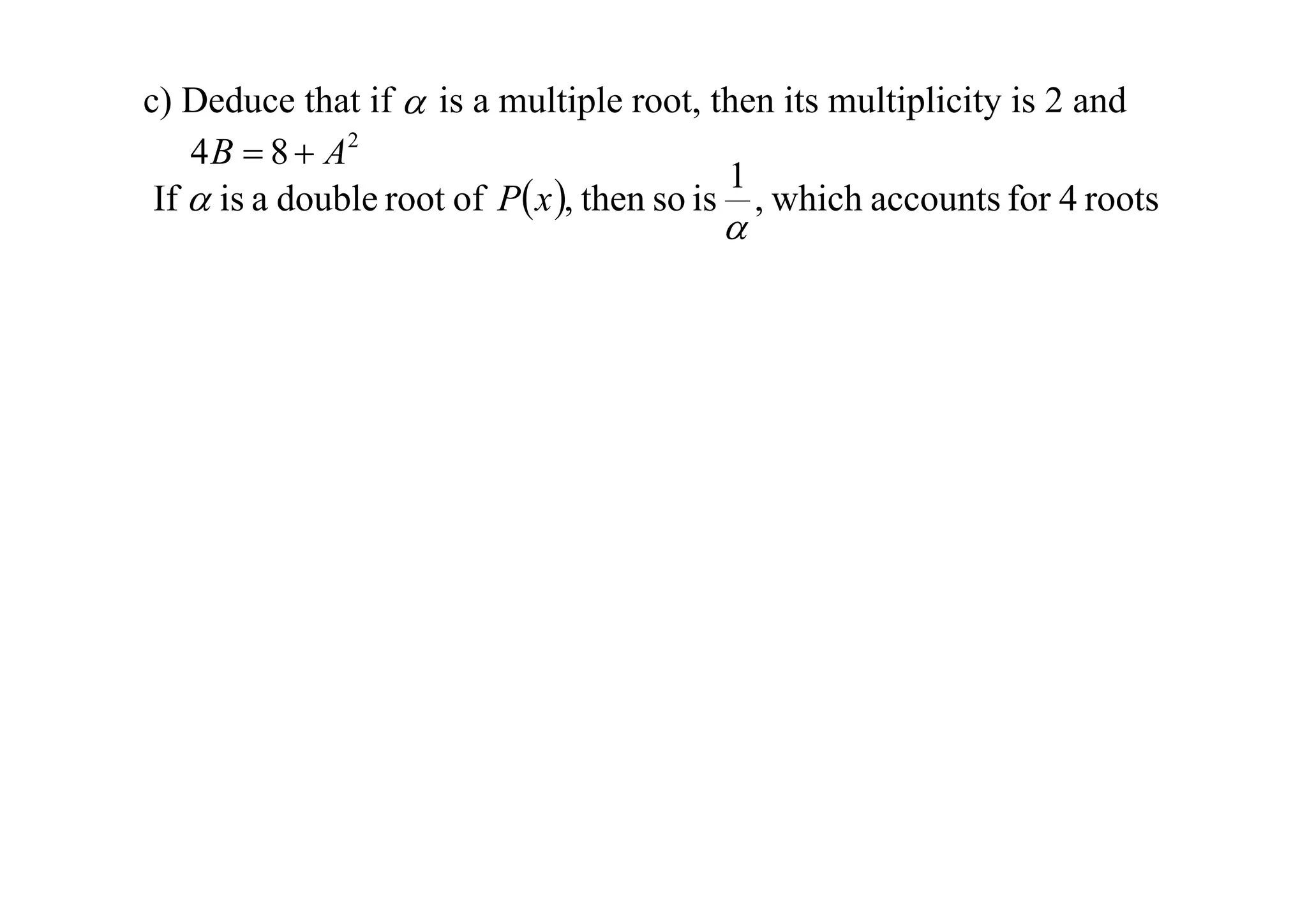
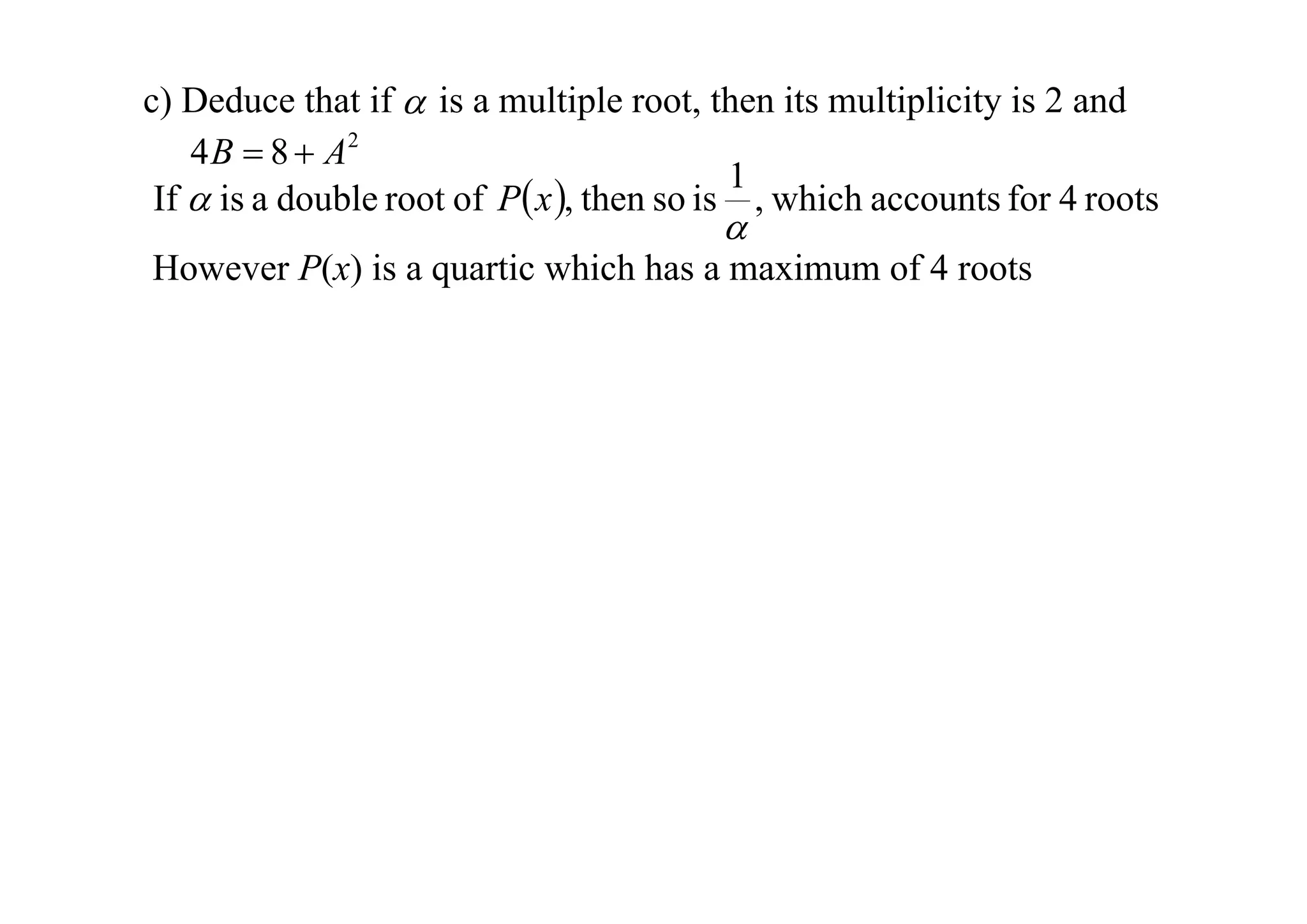
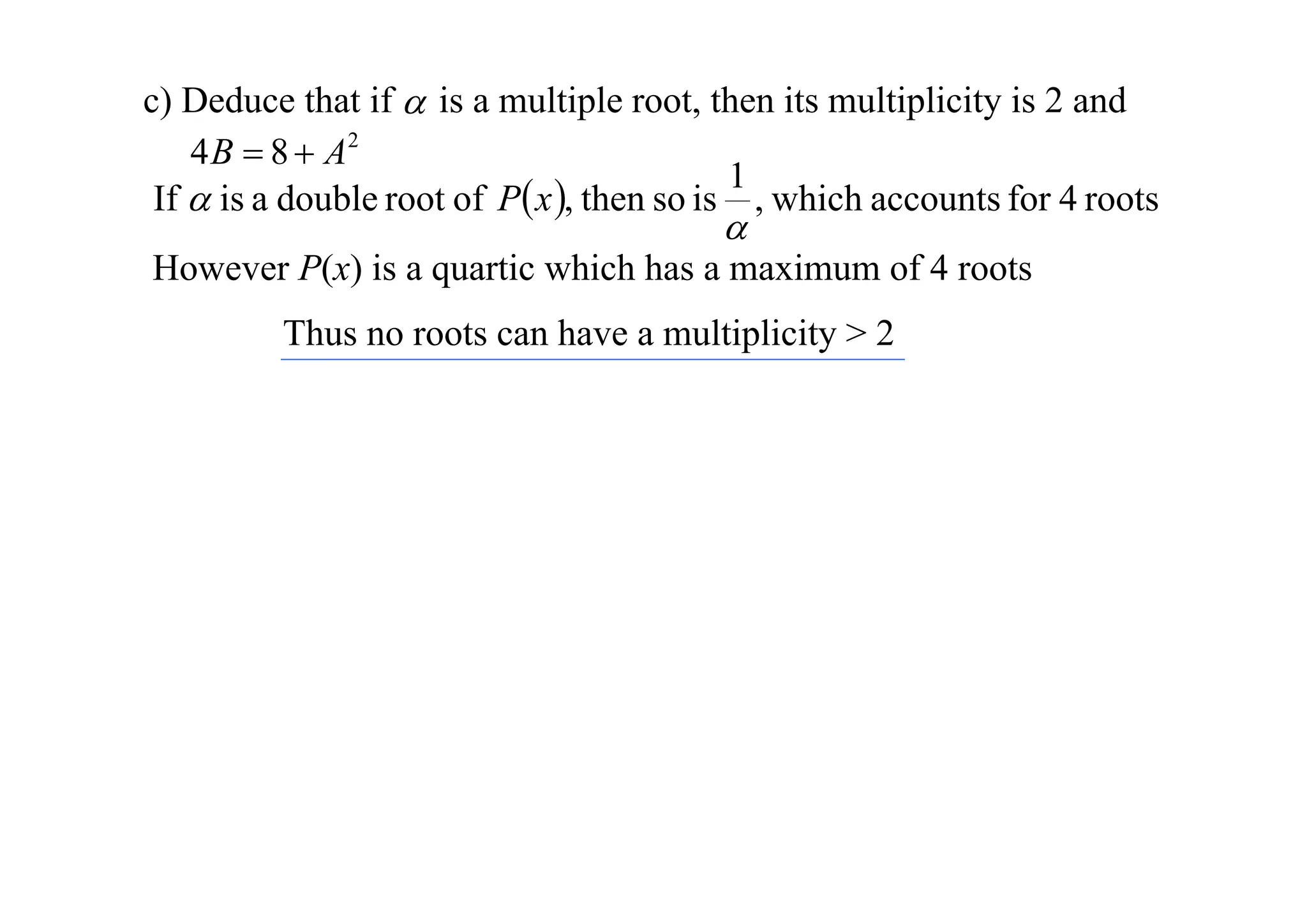
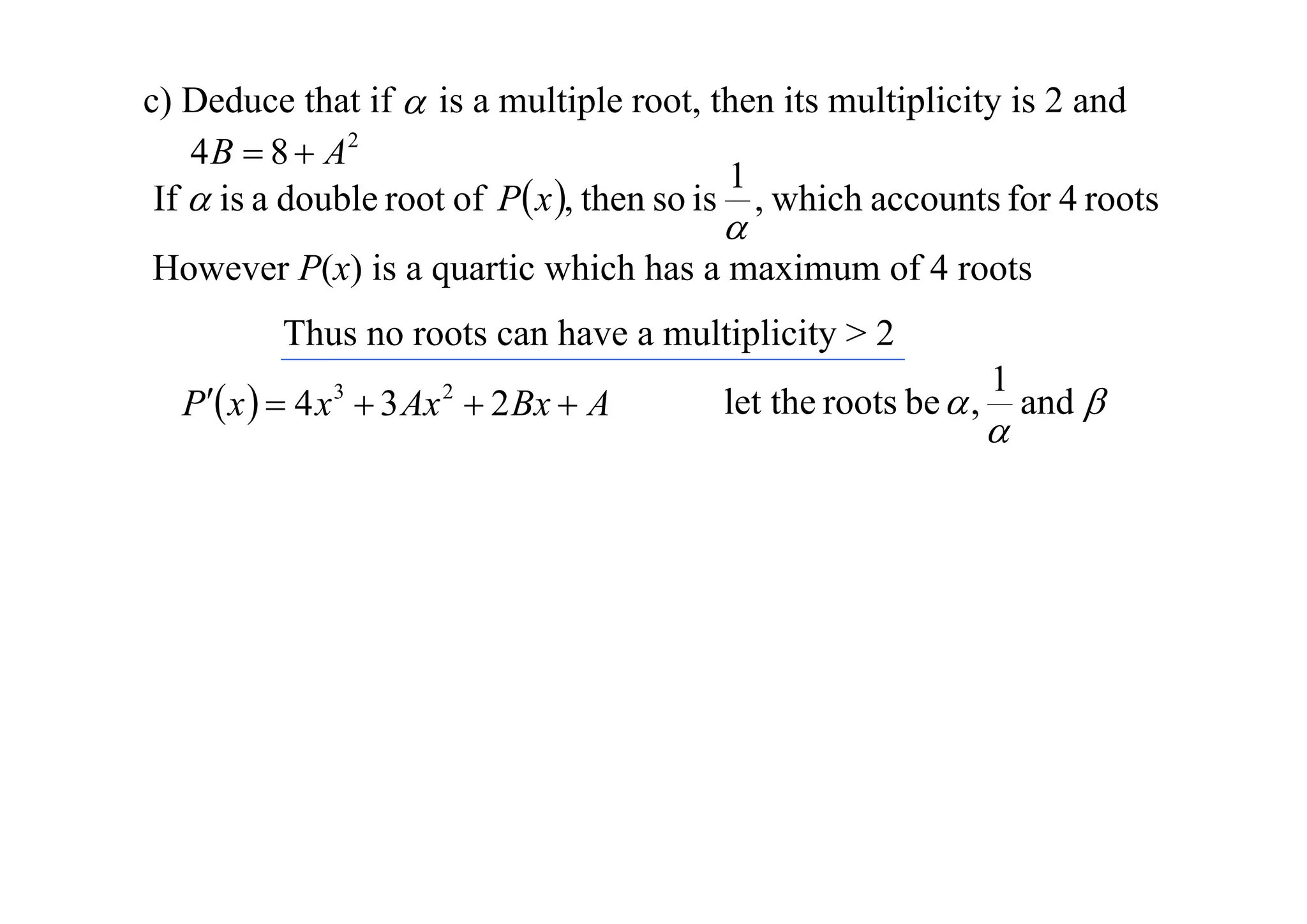
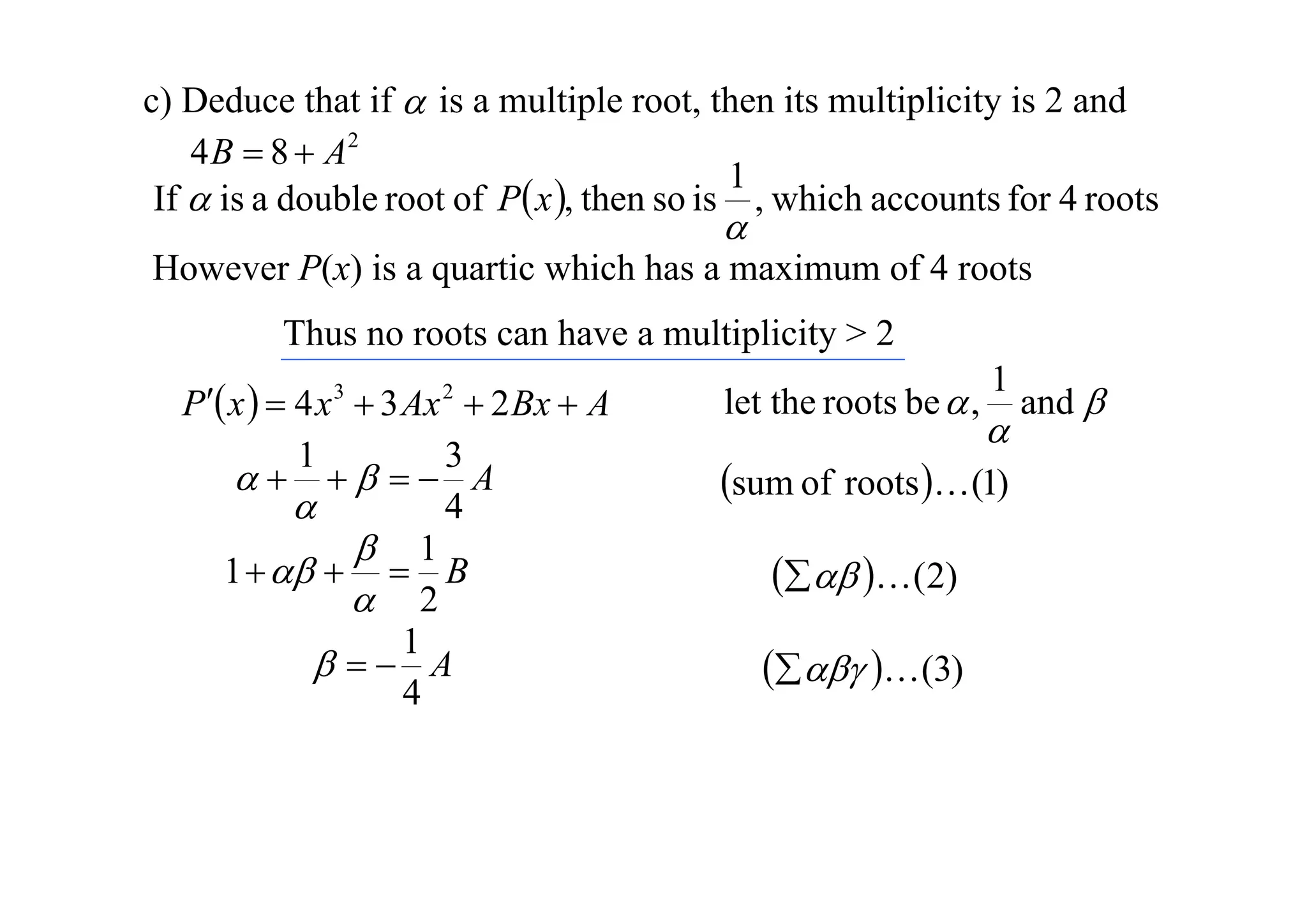
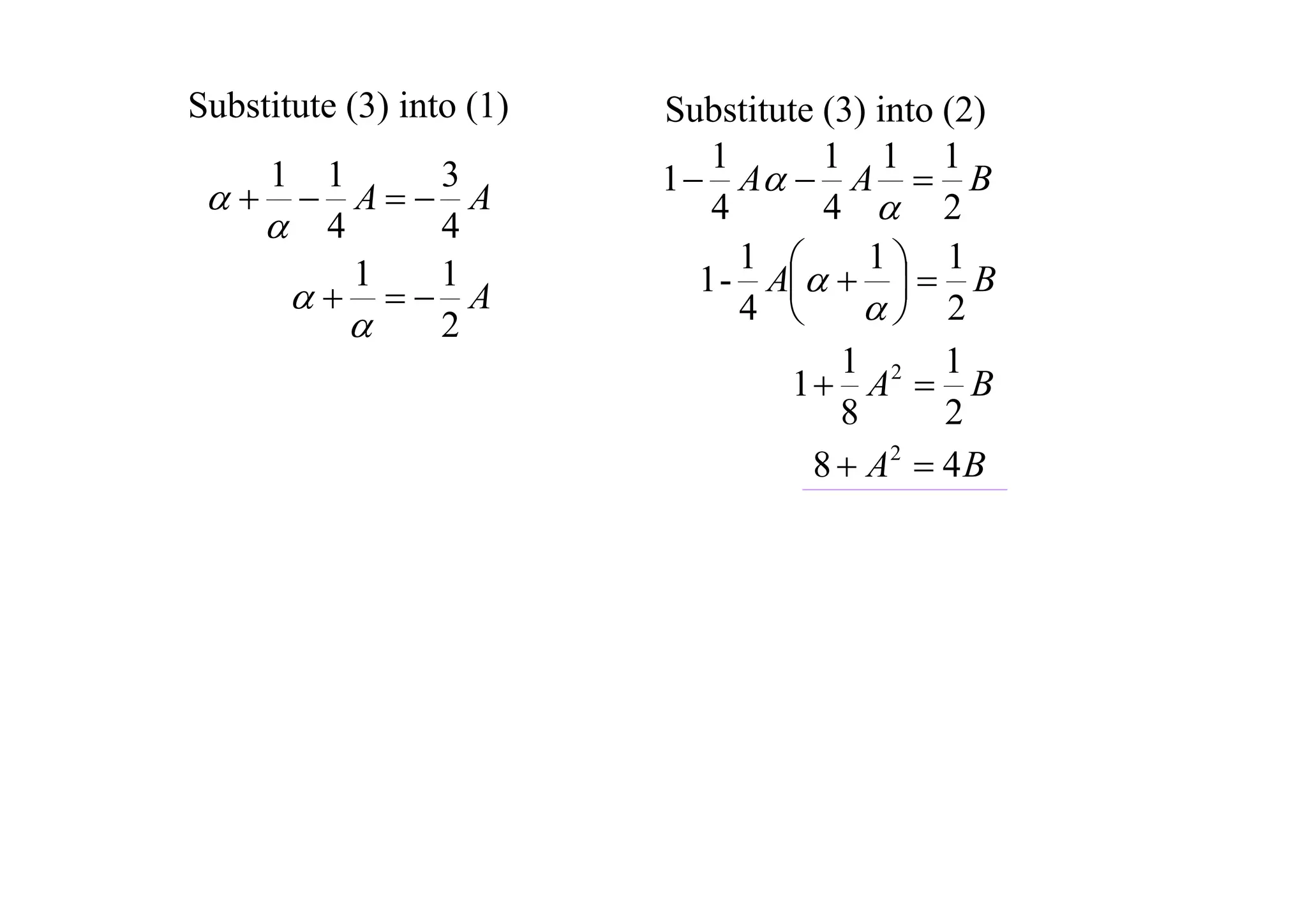
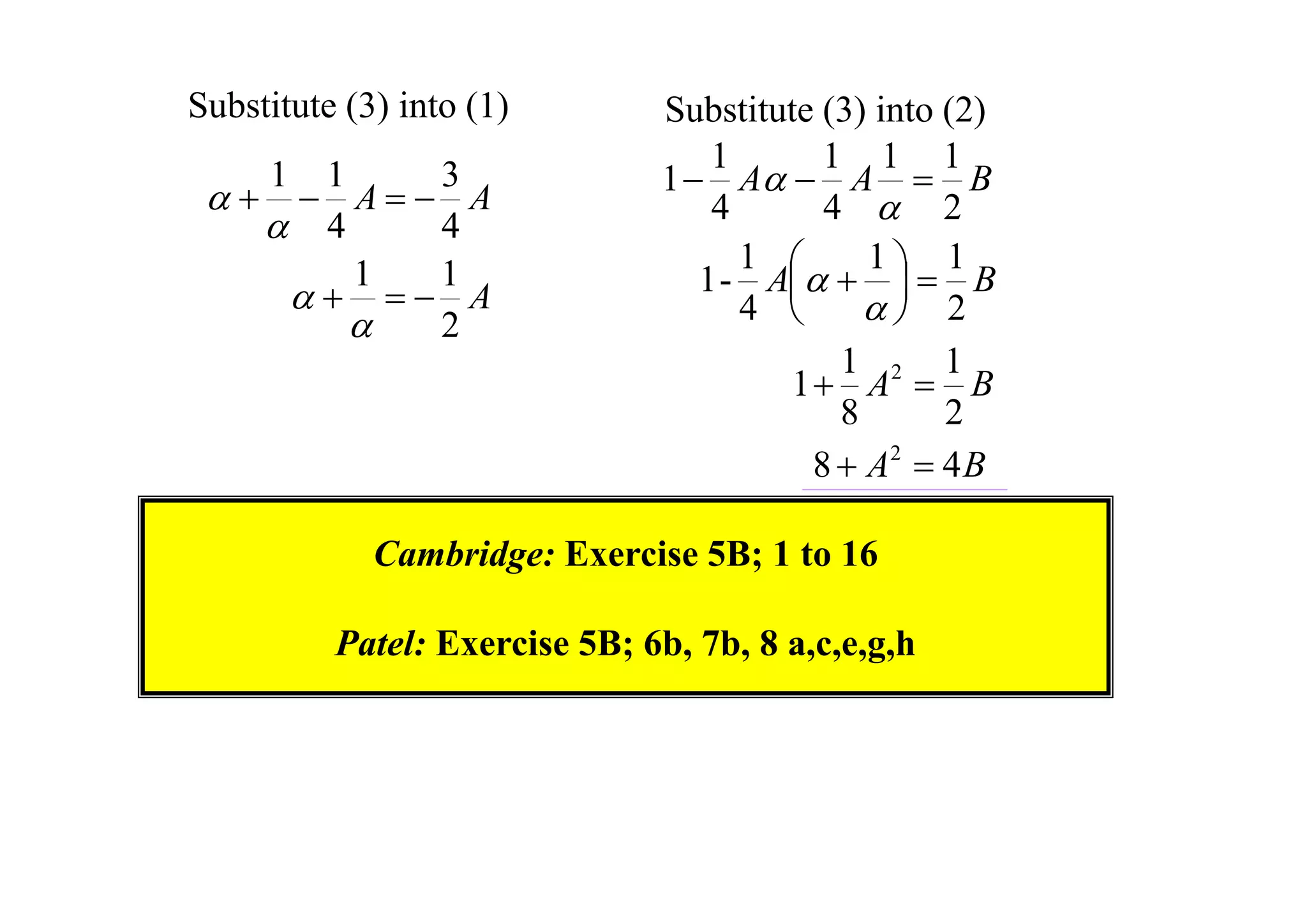
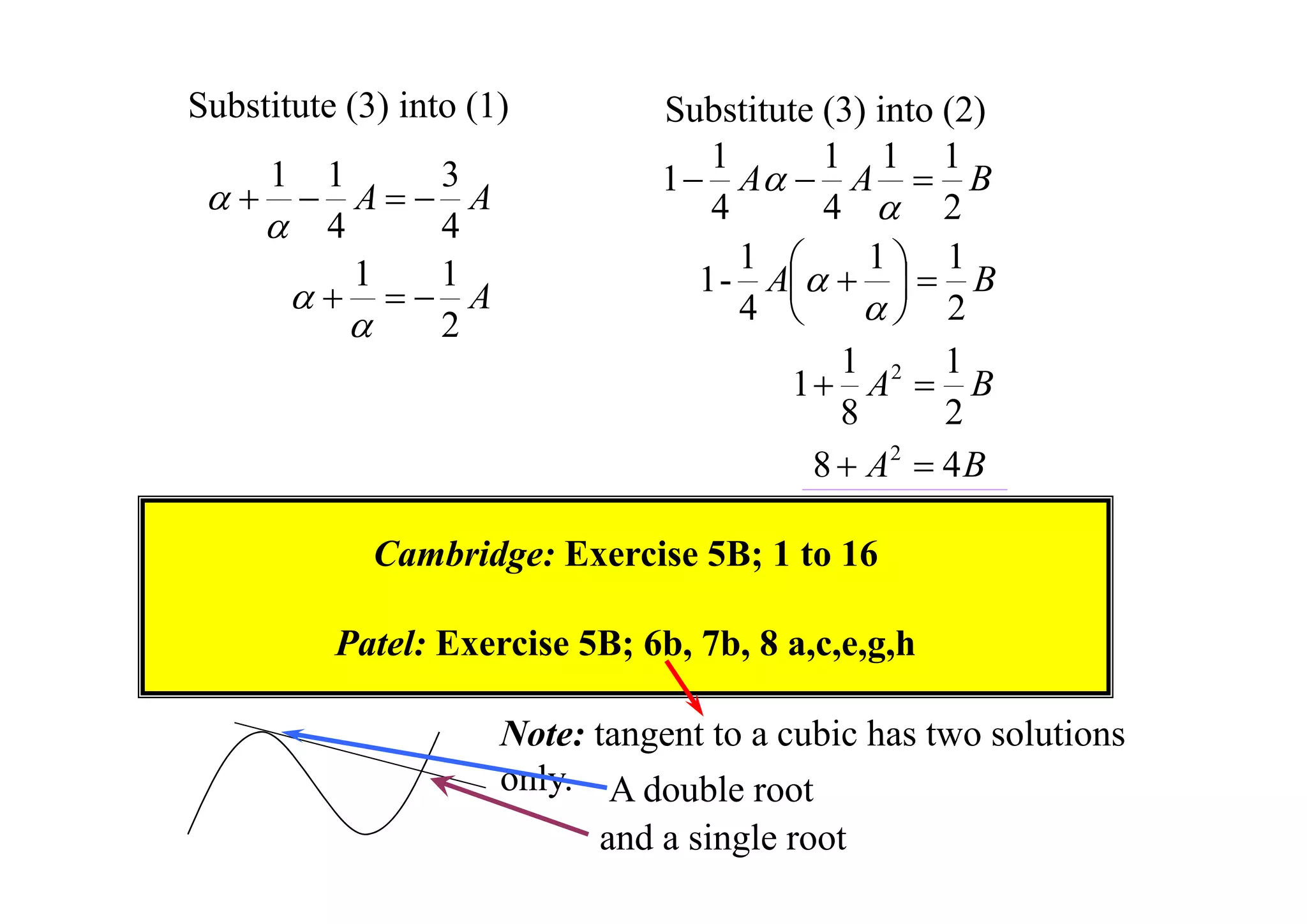
The document discusses properties of polynomials with multiple roots. It first proves that if a polynomial P(x) has a root x = a of multiplicity m, then the derivative of P(x), P'(x), will have a root x = a of multiplicity m-1. It then provides an example of solving a cubic equation given it has a double root. Finally, it examines a quartic polynomial and shows that its root α cannot be 0, 1, or -1, and that 1/























































![02[anal add math cd]](https://cdn.slidesharecdn.com/ss_thumbnails/02analaddmathcd-150416042529-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)











































