Downloaded 334 times

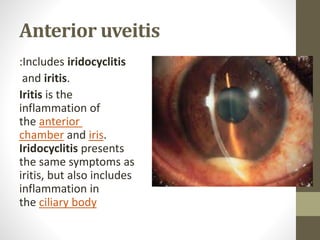
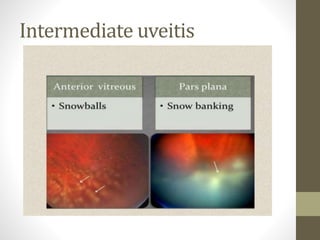














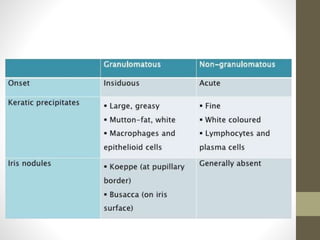









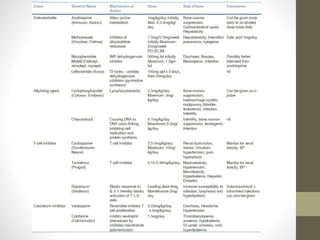







This document provides an overview of uveitis, including its definitions, classifications (anterior, intermediate, and posterior uveitis), clinical presentations, and associated systemic diseases. It discusses diagnostic investigations, treatments—primarily corticosteroids and immunosuppressants—and emphasizes the importance of addressing complications such as cystoid macular edema. Additionally, the document highlights the role of various therapies and management strategies to relieve pain and prevent visual loss.