INTRODUCTION OF UVEITIS
•Inflammation of the uvea.
• Twentieth century referred ‘‘ophthalmia.”
• Pigmented layer that lies between inner retina and
outer sclera and cornea.
• Uvea consists of middle layer of pigmented vascular
structures of the eye,
• Includes the iris, ciliary body, and choroid.
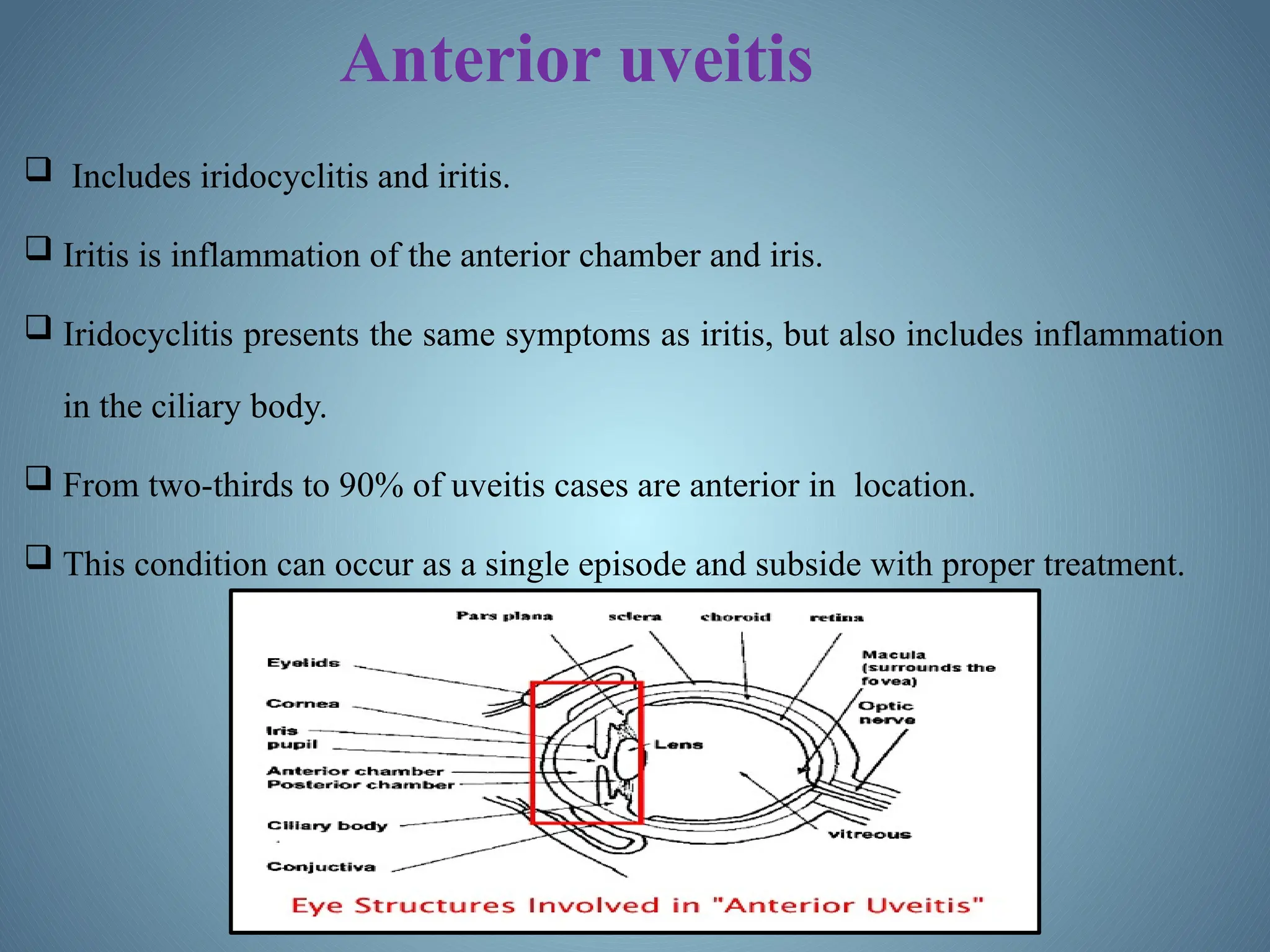
Anterior uveitis
Includesiridocyclitis and iritis.
Iritis is inflammation of the anterior chamber and iris.
Iridocyclitis presents the same symptoms as iritis, but also includes inflammation
in the ciliary body.
From two-thirds to 90% of uveitis cases are anterior in location.
This condition can occur as a single episode and subside with proper treatment.
15.
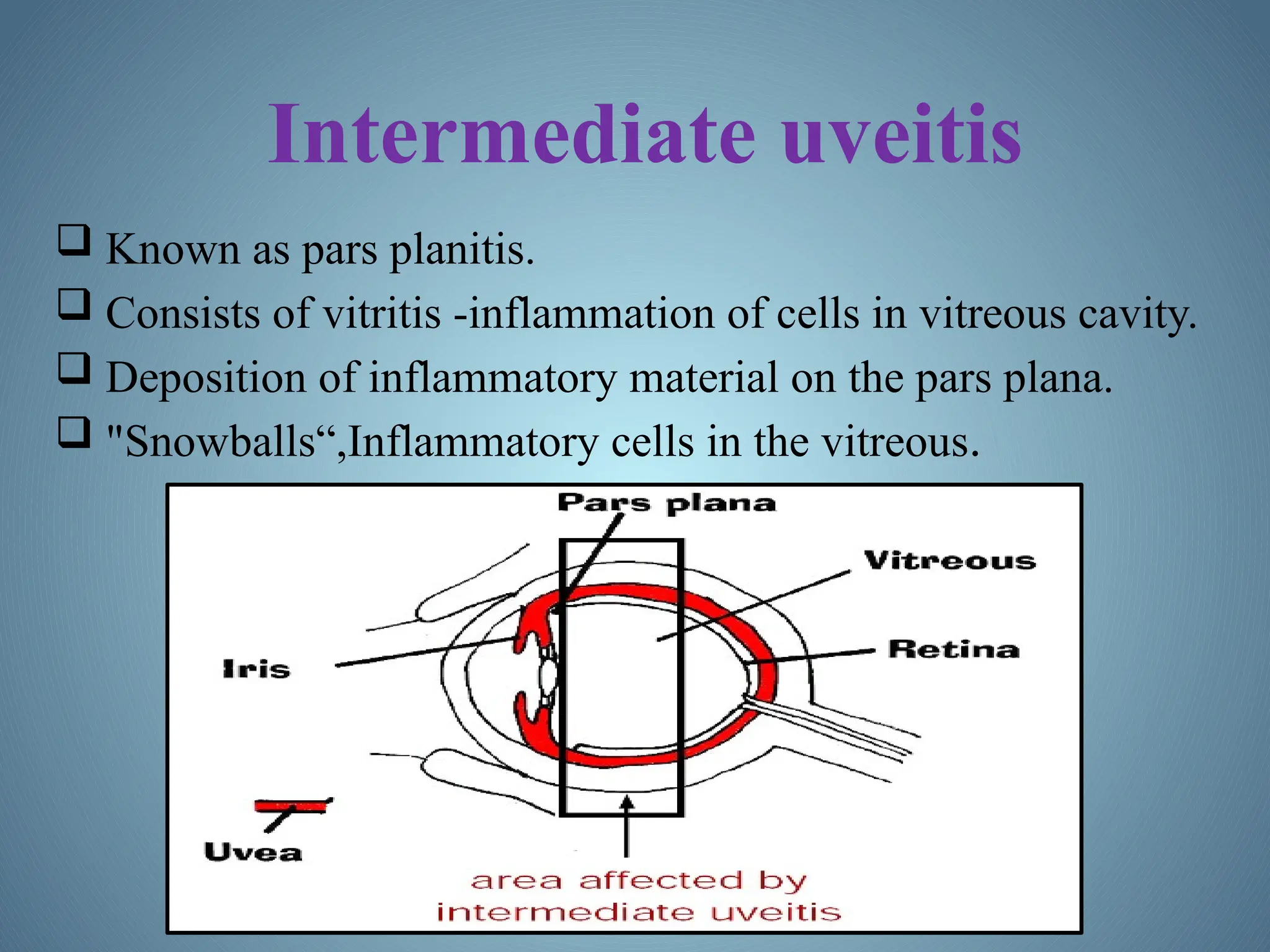
Intermediate uveitis
Knownas pars planitis.
Consists of vitritis -inflammation of cells in vitreous cavity.
Deposition of inflammatory material on the pars plana.
"Snowballs“,Inflammatory cells in the vitreous.
SYMPTOMS AND SIGNS
Anterior uveitis
Burning.
Redness.
Blurred vision.
Headaches.
Irregular pupil.
Eye pain.
Photophobia or sensitivity to light.
Floaters, which are dark spots that float in the visual field.
Drug related sideeffects
Rifabutin, a derivative of Rifampin has been
shown to cause uveitis.
Quinolones especially Moxifloxacin may lead
to uveitis.
All of the widely administered vaccines have
been reported to cause uveitis.
Immunologic factors
UveitisIs Driven By Th17t Cell Sub-population That Bear T-cell
Receptors Specific For Proteins Found In The Eye.
Not Detected Centrally Whether Due To Ocular Antigen Not Being Presented In
The Thymus.
Autoreactive T Cells Must Normally Be Held In Check By The Suppressive
Environment Produced By Microglia And Dendritic Cells In The Eye.
These Cells Produce Large Amounts Of TGF Beta And Other
Suppressive Cytokines,
Including IL-10, To Prevent Damage To The Eye By Reducing Inflammation
And Causing T Cells To Differentiate To Inducible T Reg Cells.
28.
Cont….
Immune stimulationby bacteria and cellular stress is normally
suppressed by myeloid suppression while inducible T reg cells
prevention and clonal expansion of the autoreactive Th1 and
Th 17 cells that possess potential to cause damage to the eye.
Infection or other causes, this balance can be upset and auto
reactive T cells allowed to proliferate and migrate to the eye.
Entry to the eye, these cells may be returned to an inducible T
reg state by the presence of IL-10 and TGF-beta from
microglia.
29.
Genetic Factors
Thecause of non-infectious uveitis is unknown.
But there are some strong genetic factors that predispose
disease onset .
Including HLA-B27 and the PTPN22 genotype.
30.
Infectious agents
Recentevidence has pointed to reactivation of herpes
simplex, varicella zoster and other viruses as
important causes.
Bacterial infection is another significant contributing
factor in developing uveitis.
31.
DIAGNOSIS
Diagnosis includesdilated fundus examination to rule out
posterior uveitis, which presents with white spots across the
retina along with retinitis and vasculitis.
Laboratory testing is usually used to diagnose specific
underlying diseases, including rheumatologic tests (e.g.
antinuclear antibody, rheumatoid factor, angiotensin converting
enzyme inhibitor) Serology for infectious diseases (e.g. Syphilis,
Toxoplasmosis, Tuberculosis).
fig. Keratic precipitates
32.
TREATMENT
What should treatmentachieve?
1. Relieve pain and discomfort.
2. Prevent sight loss due to the disease or its
complications.
3. Treat the cause of the disease where possible, that is,
treat the inflammation.
The drugs used to treat uveitis fall into 3 main groups.
1) Steroids
2) Immunosuppressant.
3) Mydriatics.
33.
STEROIDS
Steroids have wideranging effects but their action may
be looked on as being anti-inflammatory and
immunosuppressant".
They are used in different forms:
• Eye drops.
• Periocular injections.
• By oral (tablets).
• Intra-venous infusion (drip).
34.
Eye Drops:
Used for Anterior Uveitis.
Drops can penetrate the part of the eye in front of the lens, where anterior uveitis occurs.
Frequency of taking the drops depending on severity of the uveitis.
Severe Cases strongest drop-every hour .
Mild inflammation weakest drop once or twice a day.
Periocular Injections:
Use of injections around the eye to deliver the steroid treatment.
In certain situations injections offer a better way than either tablets or drops.
They are used along with other forms of treatment.
Situations where injections are used include:
• Severe cases of anterior uveitis which can not be controlled by drops alone.
• Intermediate uveitis.
35.
Systemic Steroids:
•Oral Steroids E.g. Prednisolone Tablet.
• The use of systemic steroids is more serious than, steroid drops because in this form
there are potentially significant side effects.
• Many different situations in which oral steroids are considered.
• If anterior uveitis is resistant to treatment with drops and injections then systemic
steroids considered.
• The main use of oral steroids is to treat posterior uveitis , panuveitis.
Dosage: Prednisolone tablet 1mg and 5mg.
Intra-venous Steroids:
E.g. Methylprednisolone.
• when rapid control of inflammation is needed high dosage of steroid needs to be
delivered quickly.
IMMUNOSUPPRESSANT
Steroids dosuppress the immune system,but there are
a different group of drugs that may be used to treat
uveitis.
These drugs tend to target the immune system more
precisely than steroids.
They are usually used in conjunction with steroids.
The main examples are:
Cyclosporine.
Azathioprine (Imuran).
Methotrexate.
Mycophenolate mofetil (cellcept).
Tacrolimus (Prograf 500).
38.
MYDRIATICS
Mydriatics have 2main aims:-
To relieve pain and light sensitivity.
To prevent sight threatening complications.
Mydriatic eye drops, Eg. Atropine and Cyclopentolate are used.
It works by "paralyzing" the muscles of the iris and the ciliary body.
It taken their effect the pupils will be dilated. This may cause
Blurring of the vision.
Useful because they help prevent complication which may occur in
anterior uveitis.