Downloaded 1,399 times

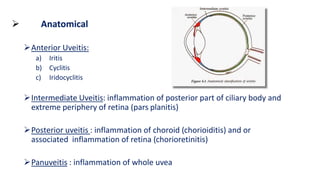























The document provides an in-depth overview of uveitis, including its classification into anterior, intermediate, posterior, and panuveitis types based on anatomical, clinical, pathological, and etiological criteria. It discusses the clinical features, complications, and treatment options, emphasizing the importance of addressing the underlying causes to prevent vision-threatening outcomes. Investigations and specific treatments for related conditions, such as tuberculosis and syphilis, are also highlighted.

















































































