Downloaded 110 times













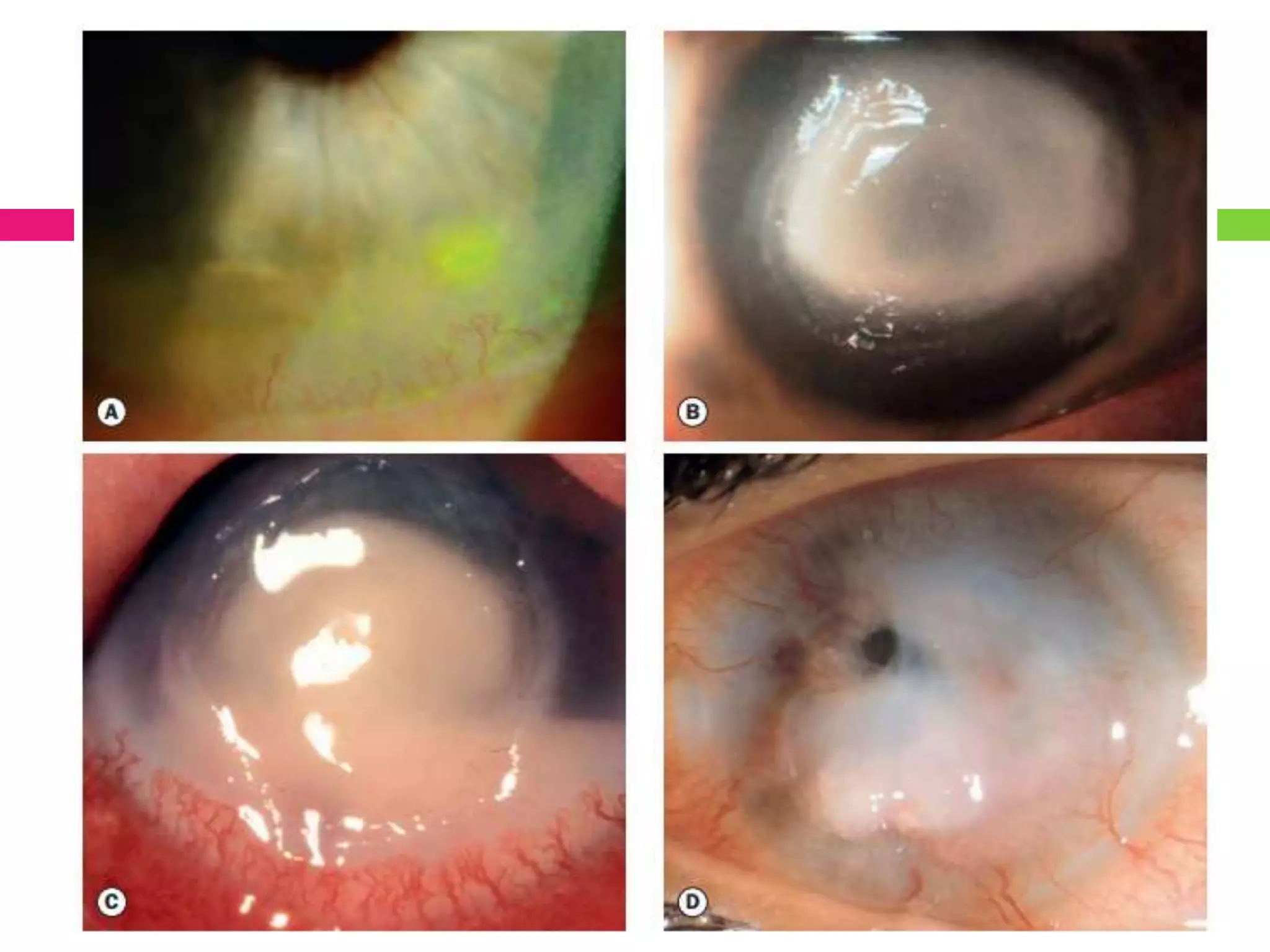



















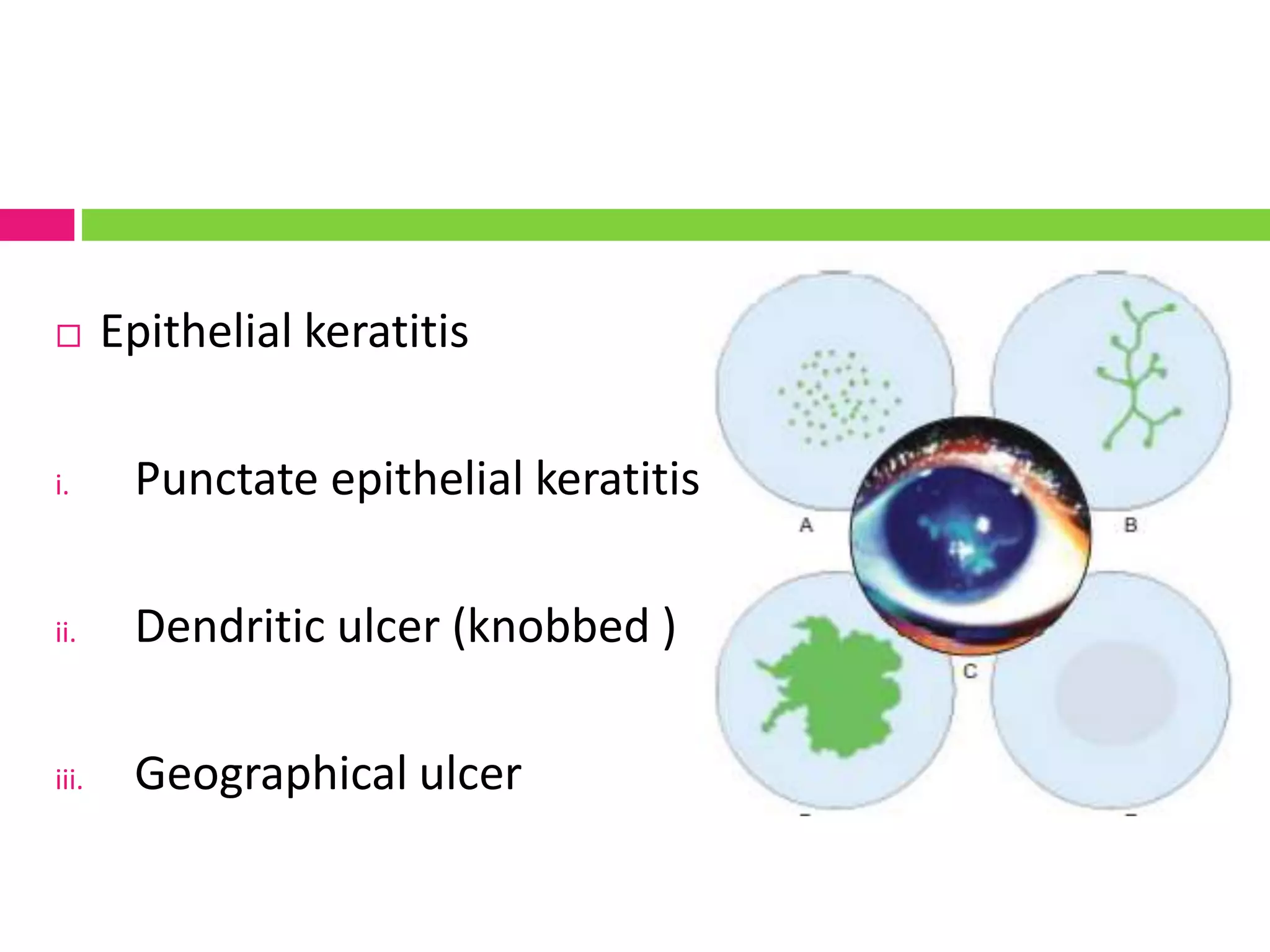













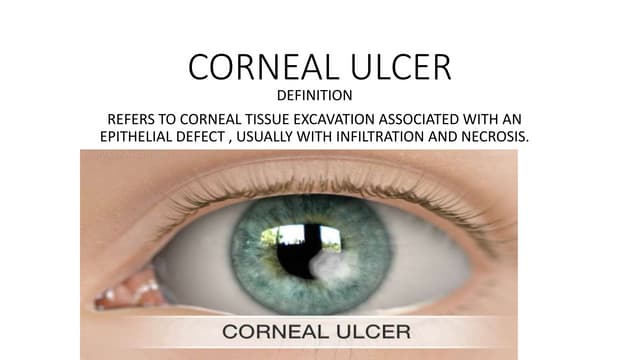
This document provides an overview of corneal ulcers, including their pathogenesis, signs and symptoms, investigations, and treatment. It discusses various types of corneal ulcers such as bacterial, viral, fungal, and protozoal ulcers. For bacterial ulcers, it outlines common causative organisms and stages of pathogenesis. Signs include infiltrate, edema, and hypopyon in the cornea. Treatment involves topical and sometimes systemic antibiotics. Viral ulcers like herpes simplex can cause epithelial dendritic ulcers or stromal keratitis. Treatment is with antiviral medications like acyclovir. Fungal ulcers are treated with antifungal eye drops and sometimes systemic antifungals.