Downloaded 894 times


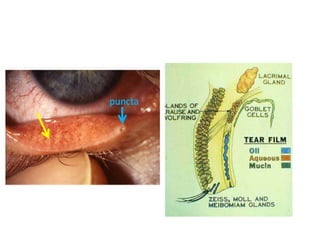

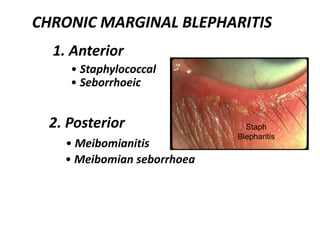

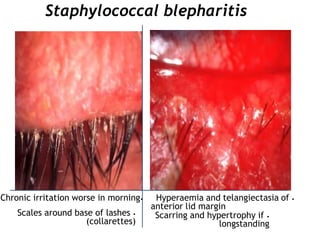
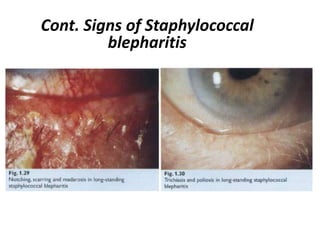
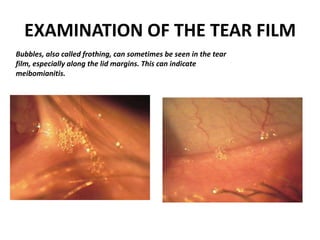

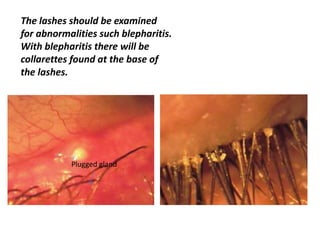


Blepharitis is a common eyelid inflammation that can be caused by bacterial infections or dry eye conditions. It is characterized by scaling or crusting of the eyelashes and eyelid margins. There are two main types - anterior blepharitis, which involves inflammation at the base of the eyelashes, and posterior blepharitis, which affects the glands of the eyelid. Symptoms include burning, irritation, tearing and worsening in the morning. Treatment focuses on eyelid hygiene through warm compresses and lid scrubs to remove scales and debris. Blepharitis can exacerbate dry eye and may cause long-term eyelid changes if left untreated. It may also increase risks of certain inflammatory



























































![BLEPHARITIS [Autosaved] group 32.pptx yyuhyyy](https://cdn.slidesharecdn.com/ss_thumbnails/blepharitisautosavedgroup32-241010163121-429a2f06-thumbnail.jpg?width=640&height=640&fit=bounds)





















![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)














