Downloaded 31 times


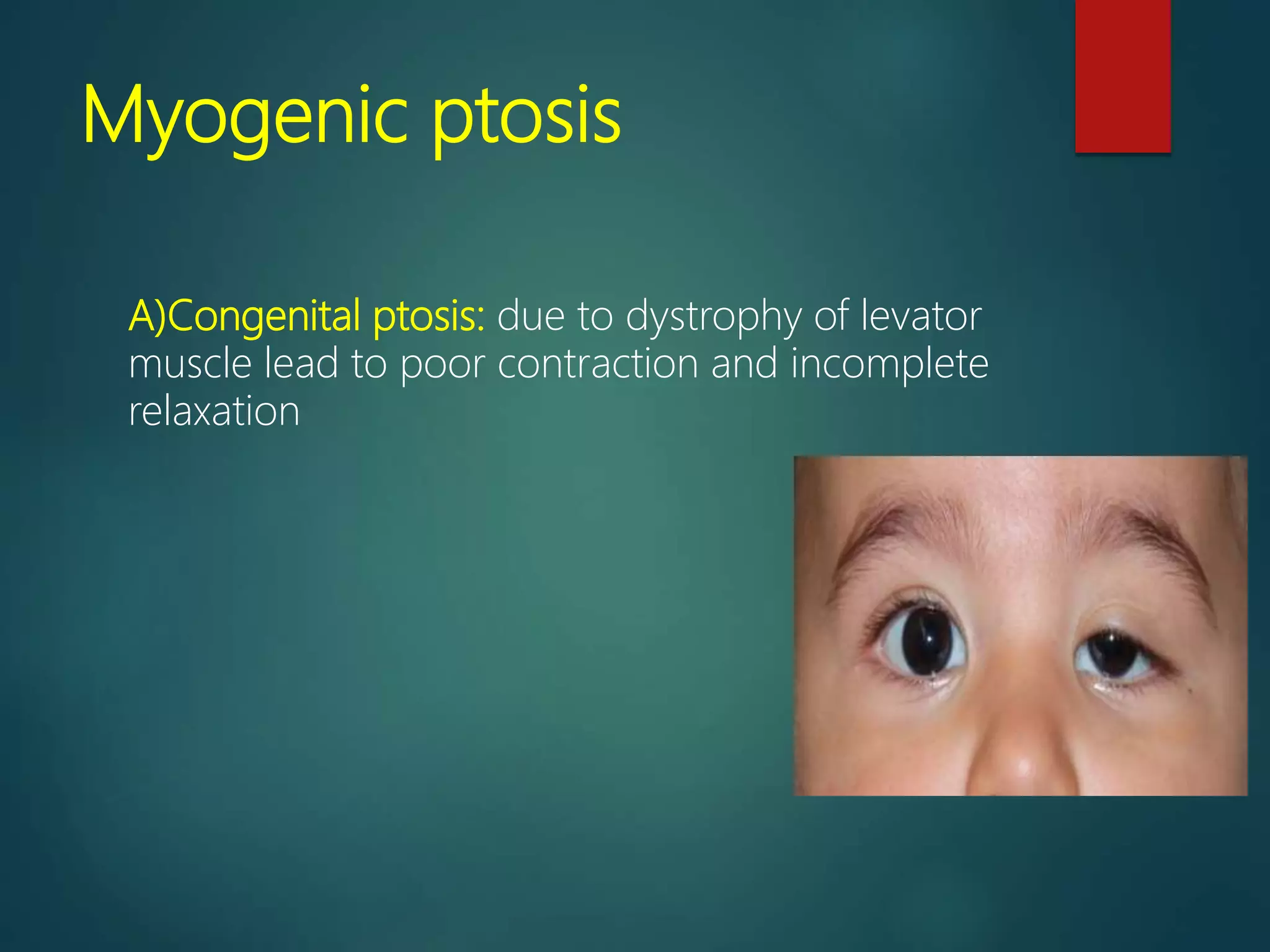



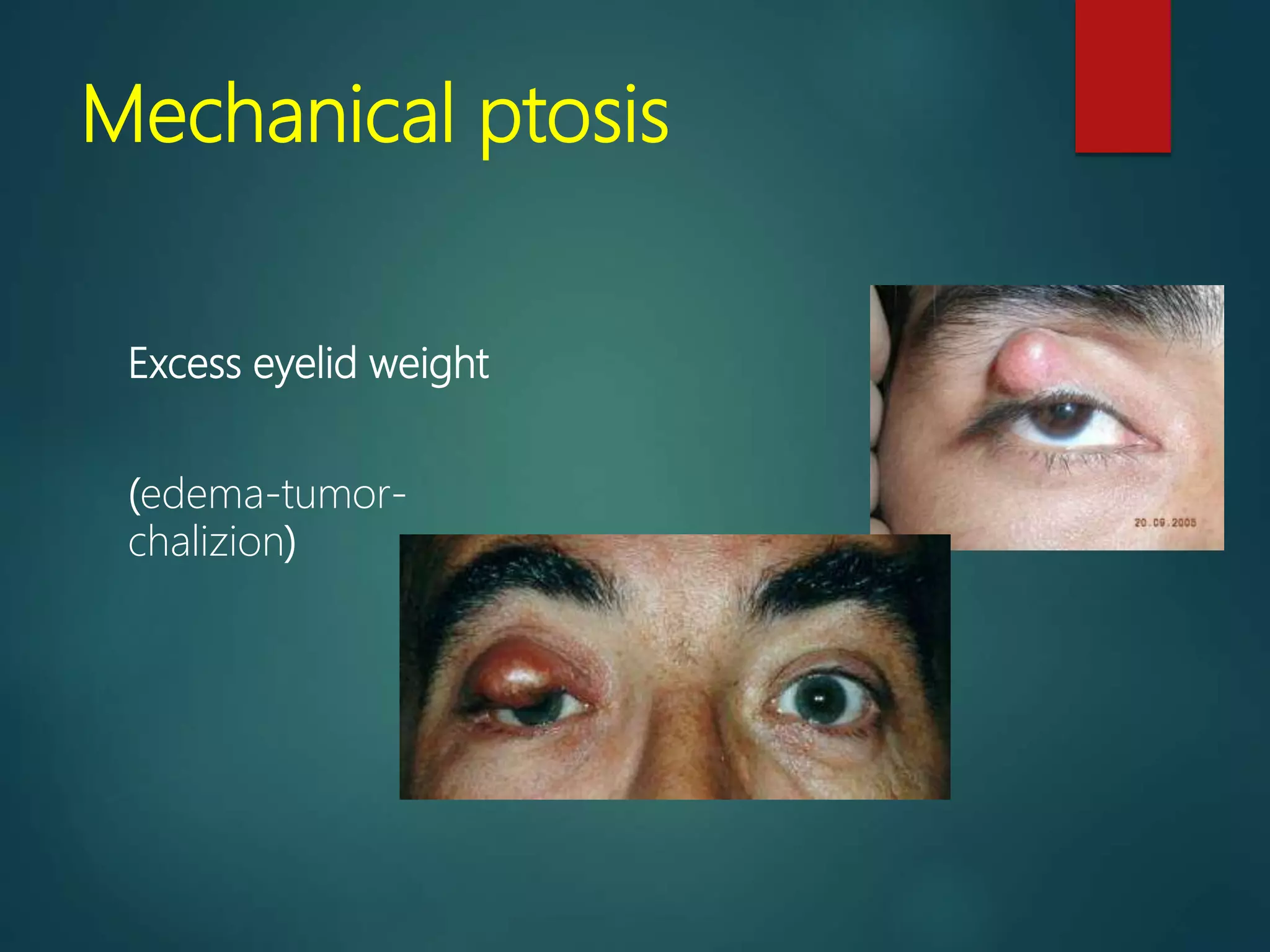
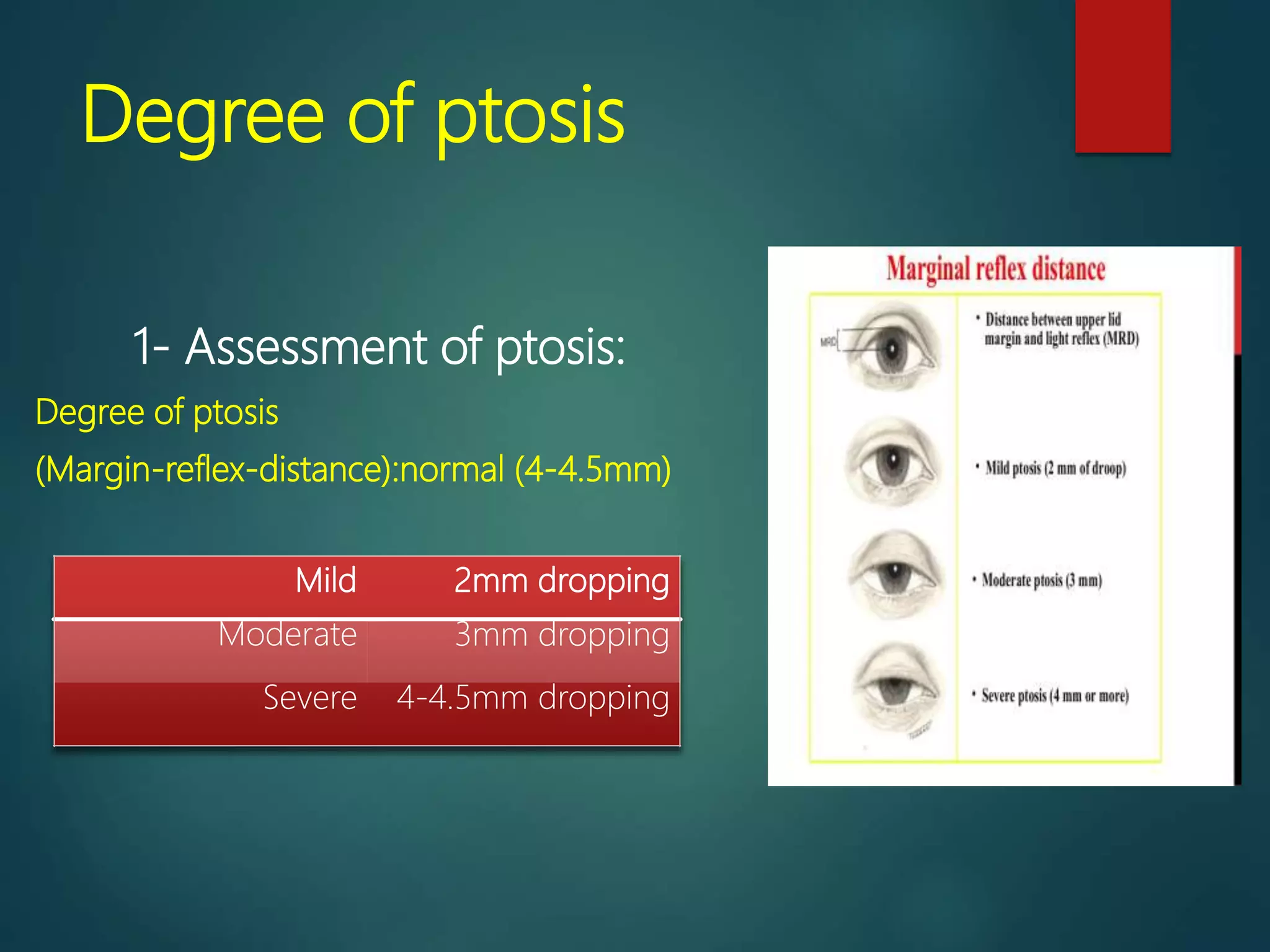


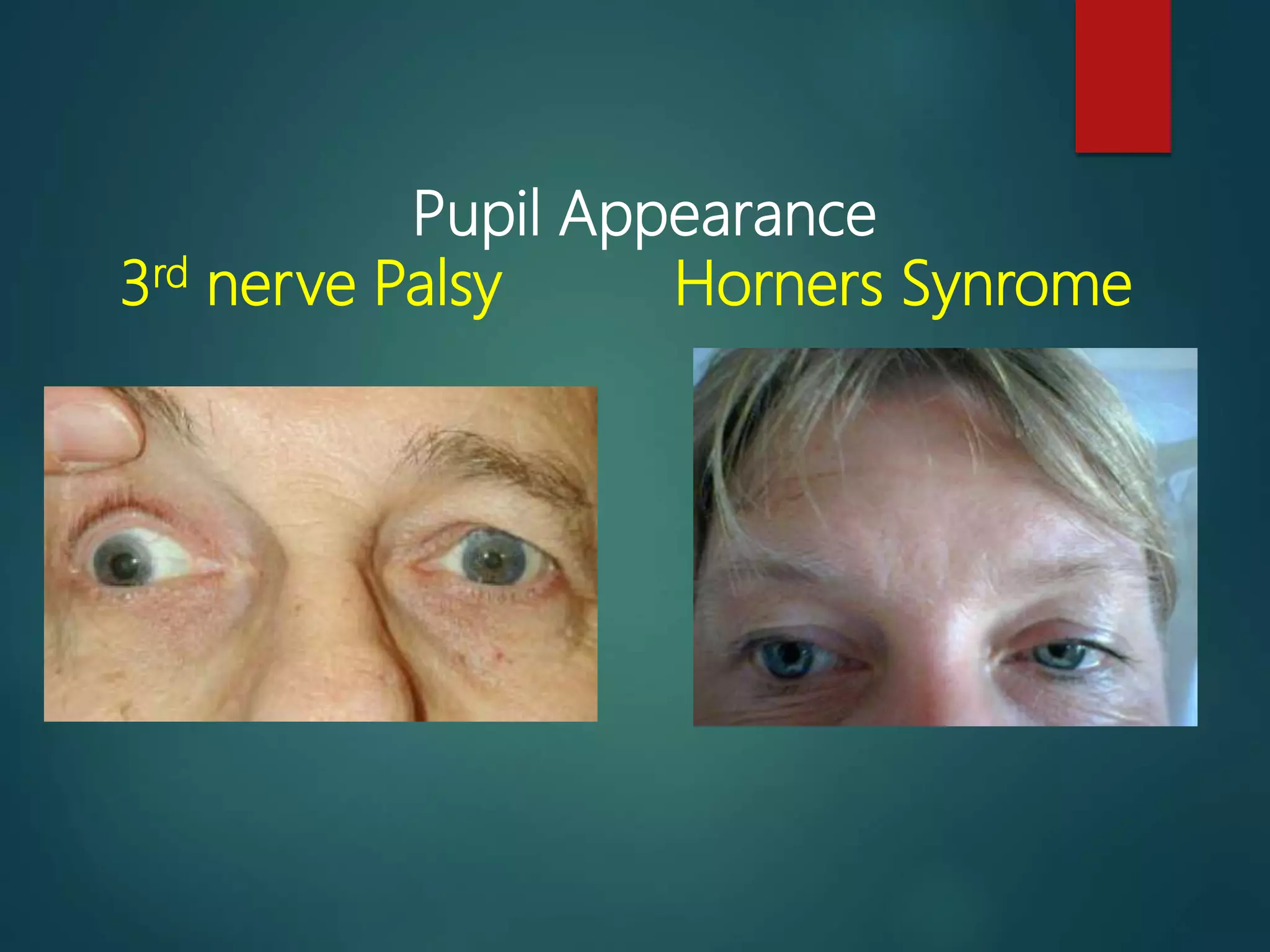
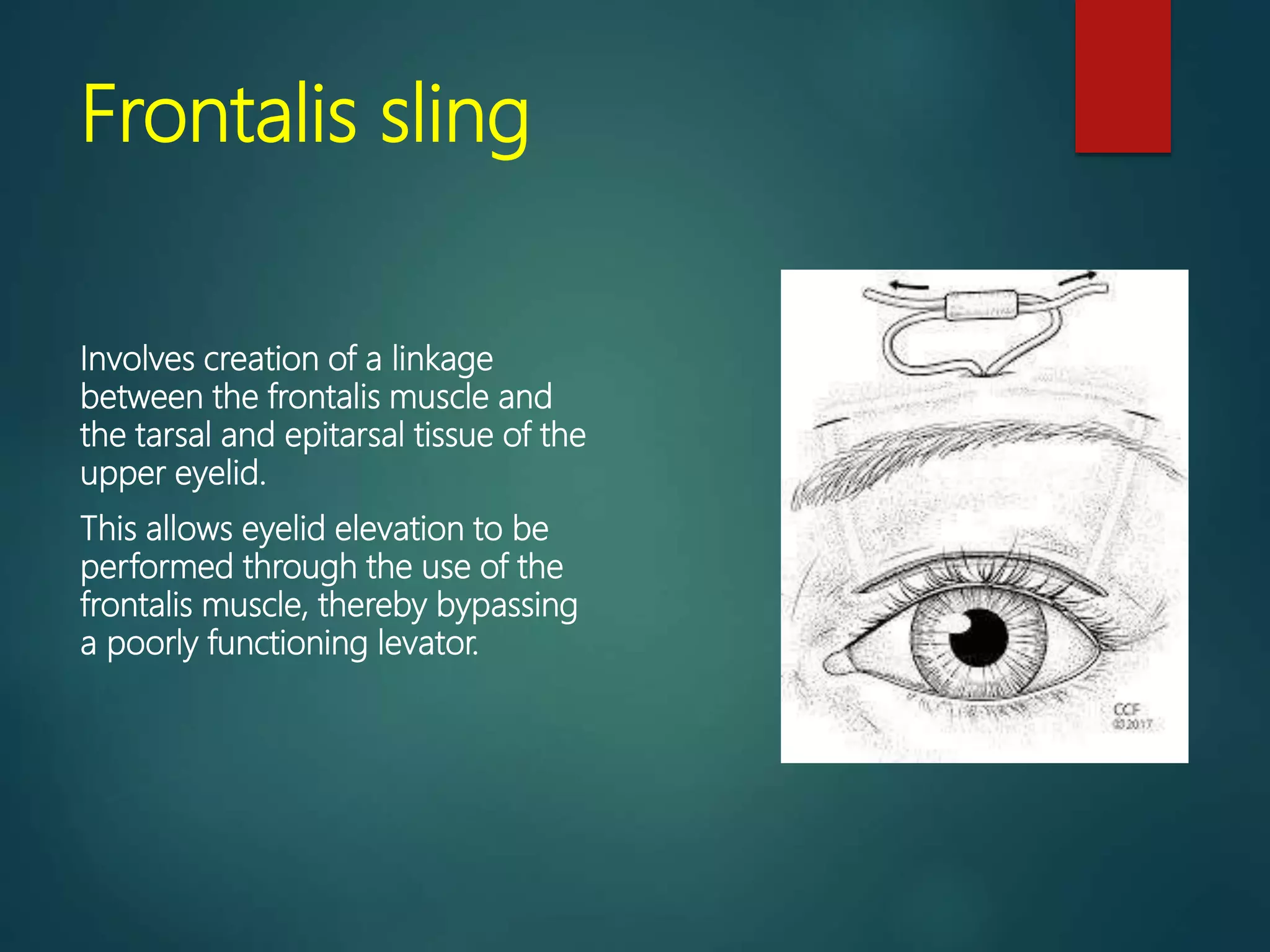




Ptosis, or drooping of the upper eyelid, can have several causes including paralysis or disease (myogenic, neurogenic), or be congenital (aponeurotic). Myogenic ptosis may be congenital due to poor levator muscle contraction/relaxation, or acquired like in myasthenia gravis where the myoneural junction is defective. Neurogenic ptosis includes third nerve palsy or Horner's syndrome. Aponeurotic ptosis includes senile or postoperative changes. Treatment depends on the cause and degree of ptosis, and may involve frontal sling surgery using the frontalis muscle, levator resection/advancement for moderate ptosis, or Whitnall sling or









































![CLINICAL EVALUATION AND MANAGEMENT OPTION OF AQUIRED PTOSIS [Autosaved]_09133...](https://cdn.slidesharecdn.com/ss_thumbnails/clinicalevaluationandmanagementoptionofaquiredptosisautosaved091336-250701164538-7d28272b-thumbnail.jpg?width=640&height=640&fit=bounds)













































