Download to read offline






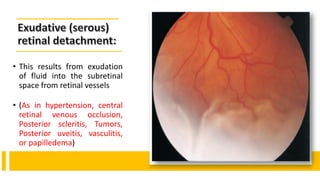
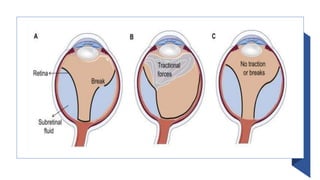

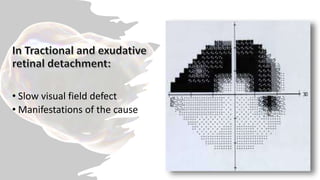
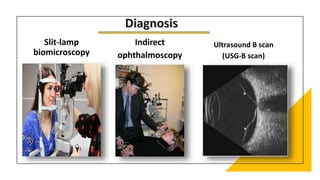




This document discusses retinal detachment, which occurs when the retina separates from the underlying tissue. The most common type, rhegmatogenous retinal detachment, results from a tear or break in the retina that allows fluid to seep in. Symptoms include floaters, visual field defects, and flashes of light. Diagnosis involves examinations of the eye and ultrasound. Treatment depends on the type but generally aims to seal retinal breaks, relieve traction, and reattach the retina using procedures like cryotherapy, laser photocoagulation, pneumatic retinopexy using gas bubbles, or vitrectomy surgery to remove the vitreous gel.























































































