Download to read offline
















































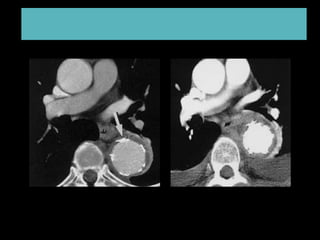






Type B aortic dissection occurs when blood flows within the aortic wall separating the layers of the media. Computed tomography angiography is useful for establishing the diagnosis by showing two distinct lumens separated by an intimal flap, and for determining the location of the primary intimal tear and extent of dissection. Initial medical management aims to control blood pressure and pain. Intervention may be indicated for complications such as persistent pain, expansion of the dissection, or impaired blood flow to organs. Both open surgical repair and endovascular techniques can be used to treat type B dissection, with endovascular options becoming more common due to lower risks.