Downloaded 19 times


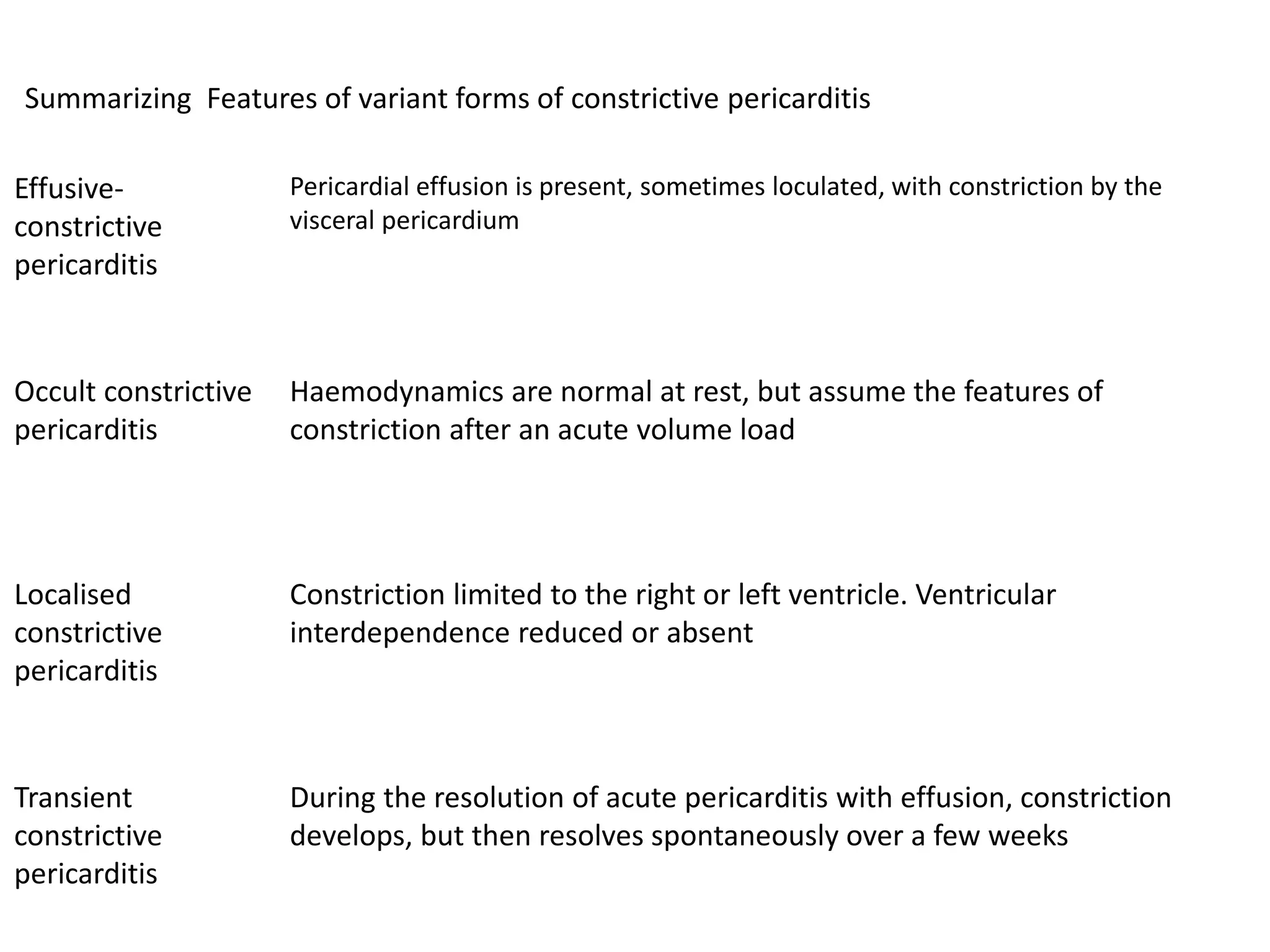




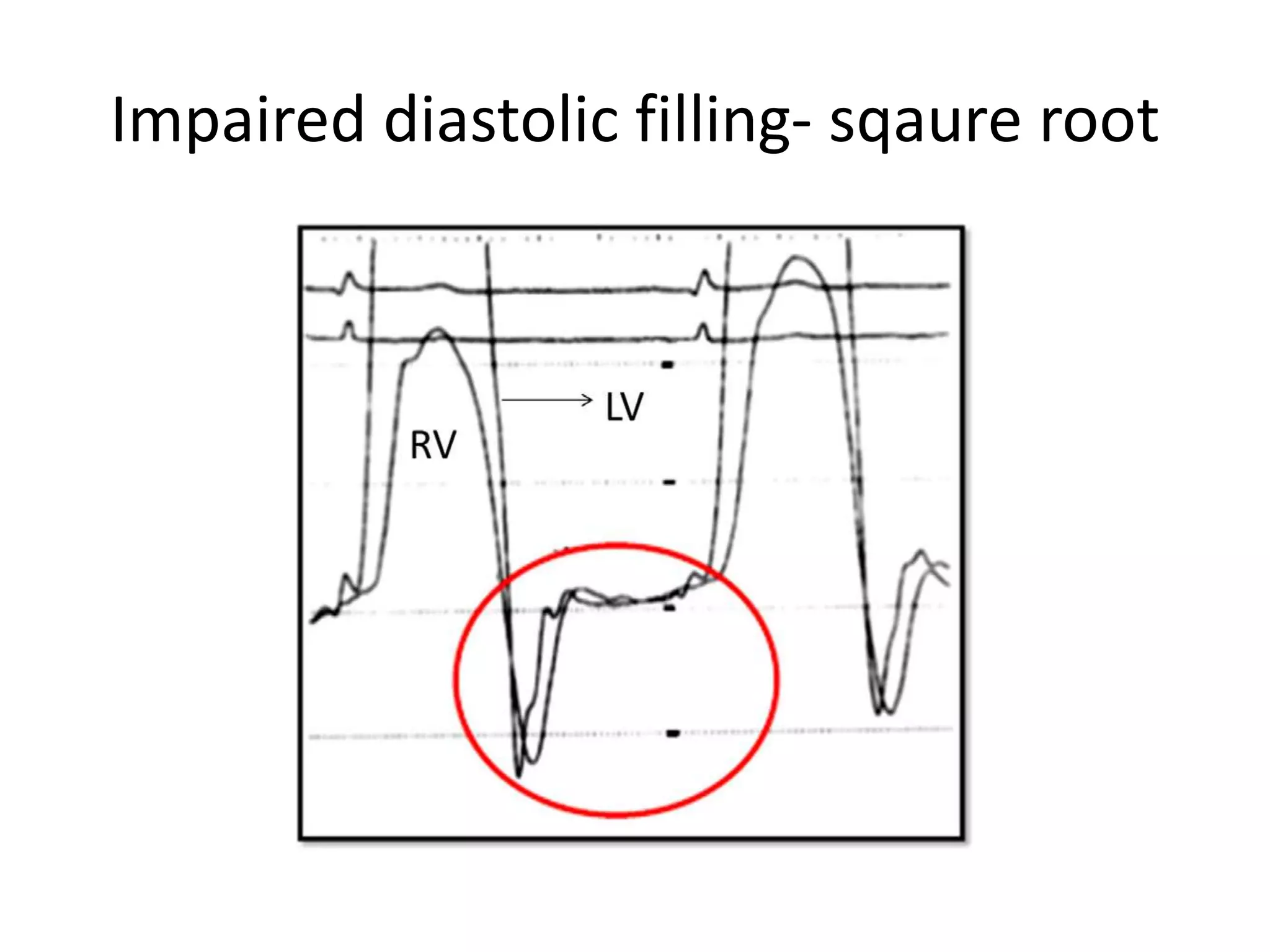







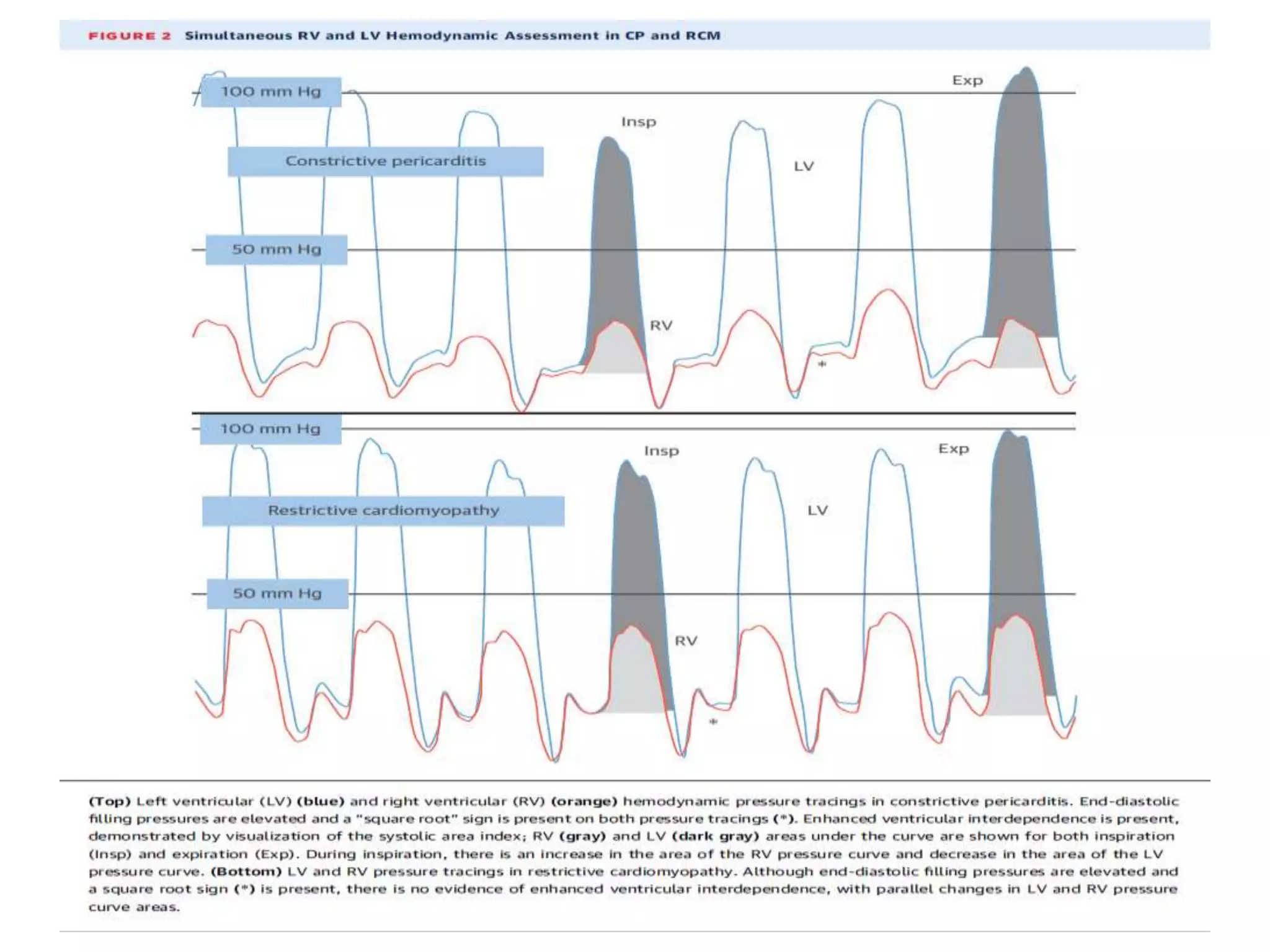
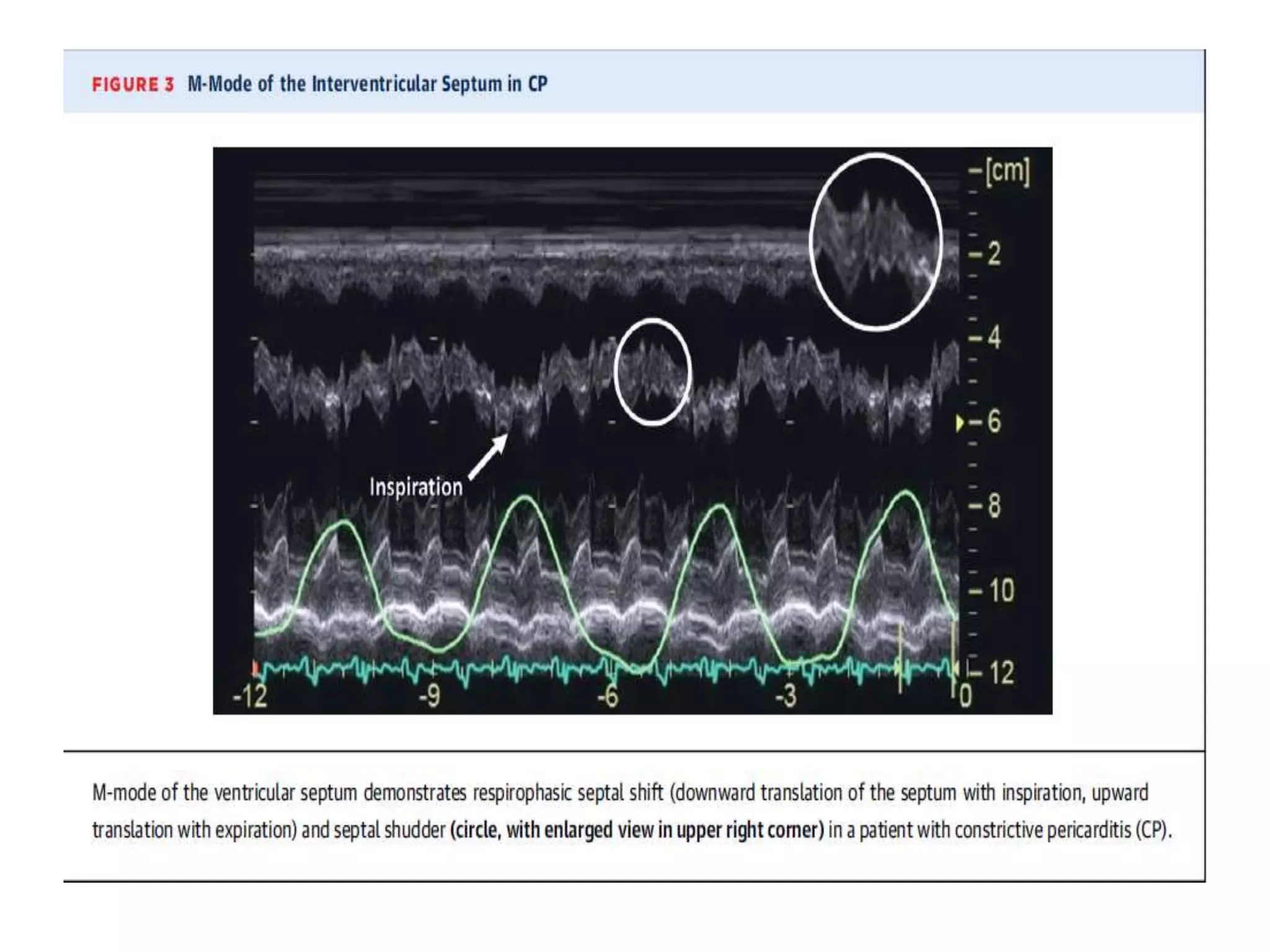
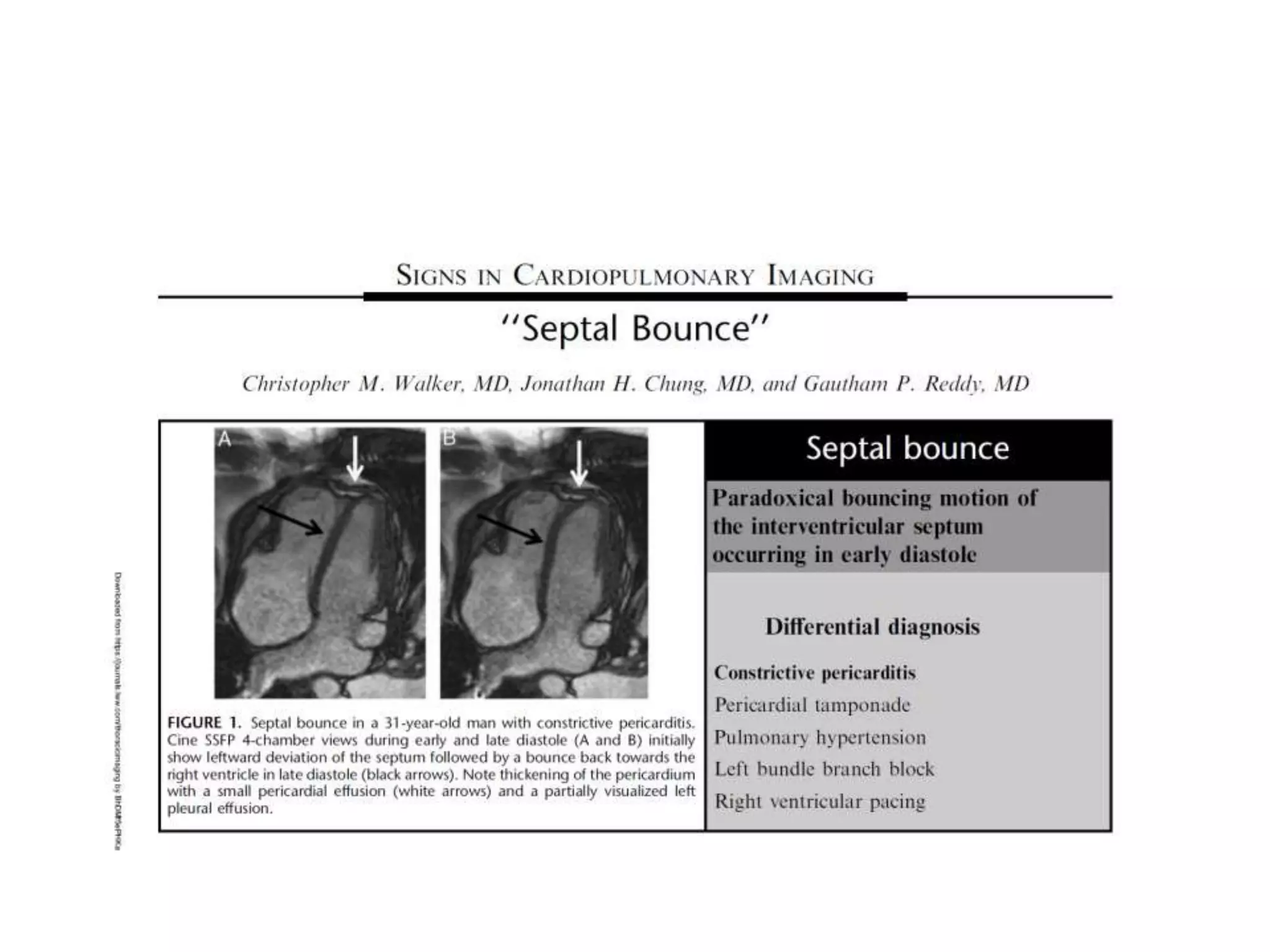







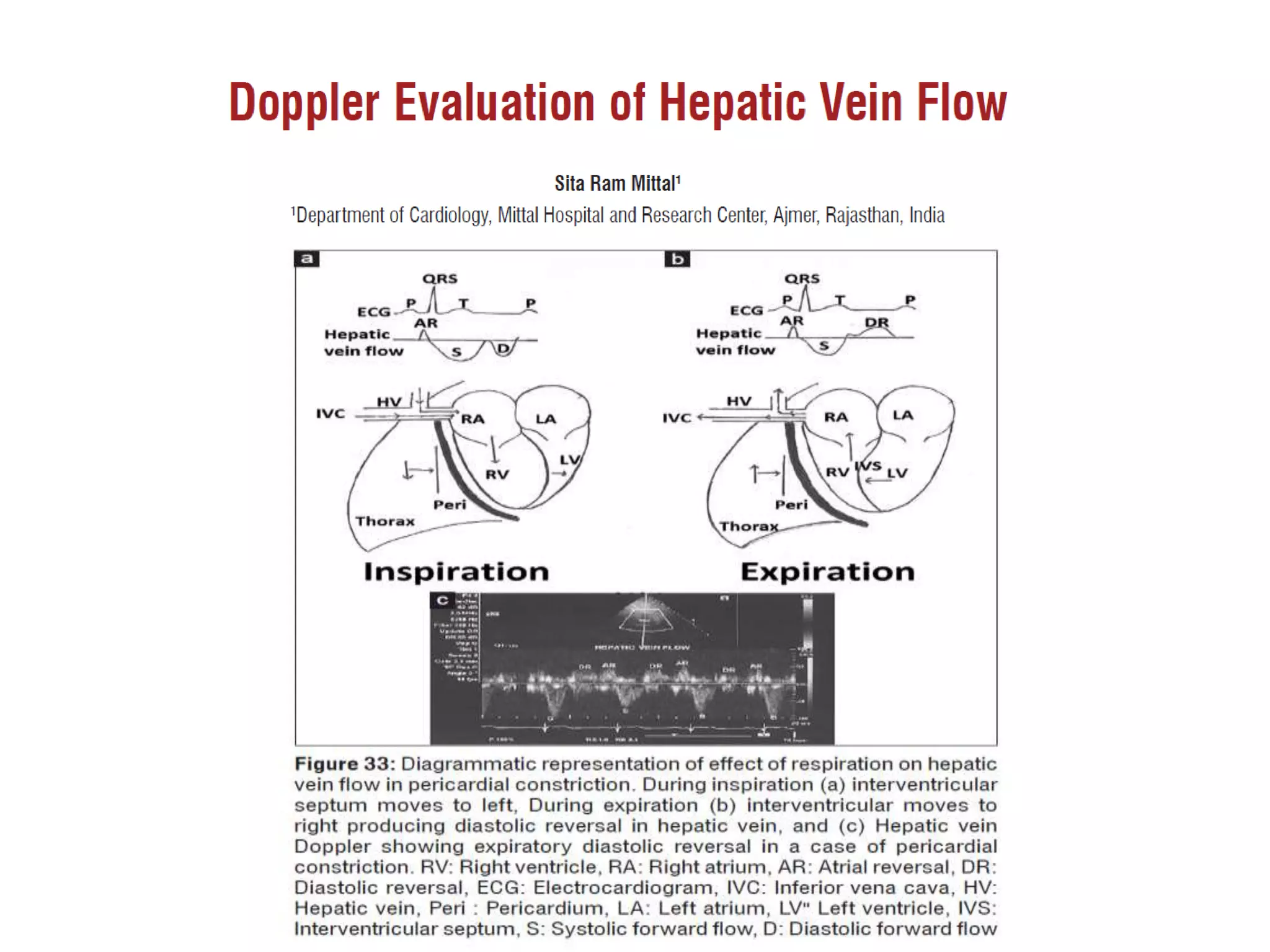


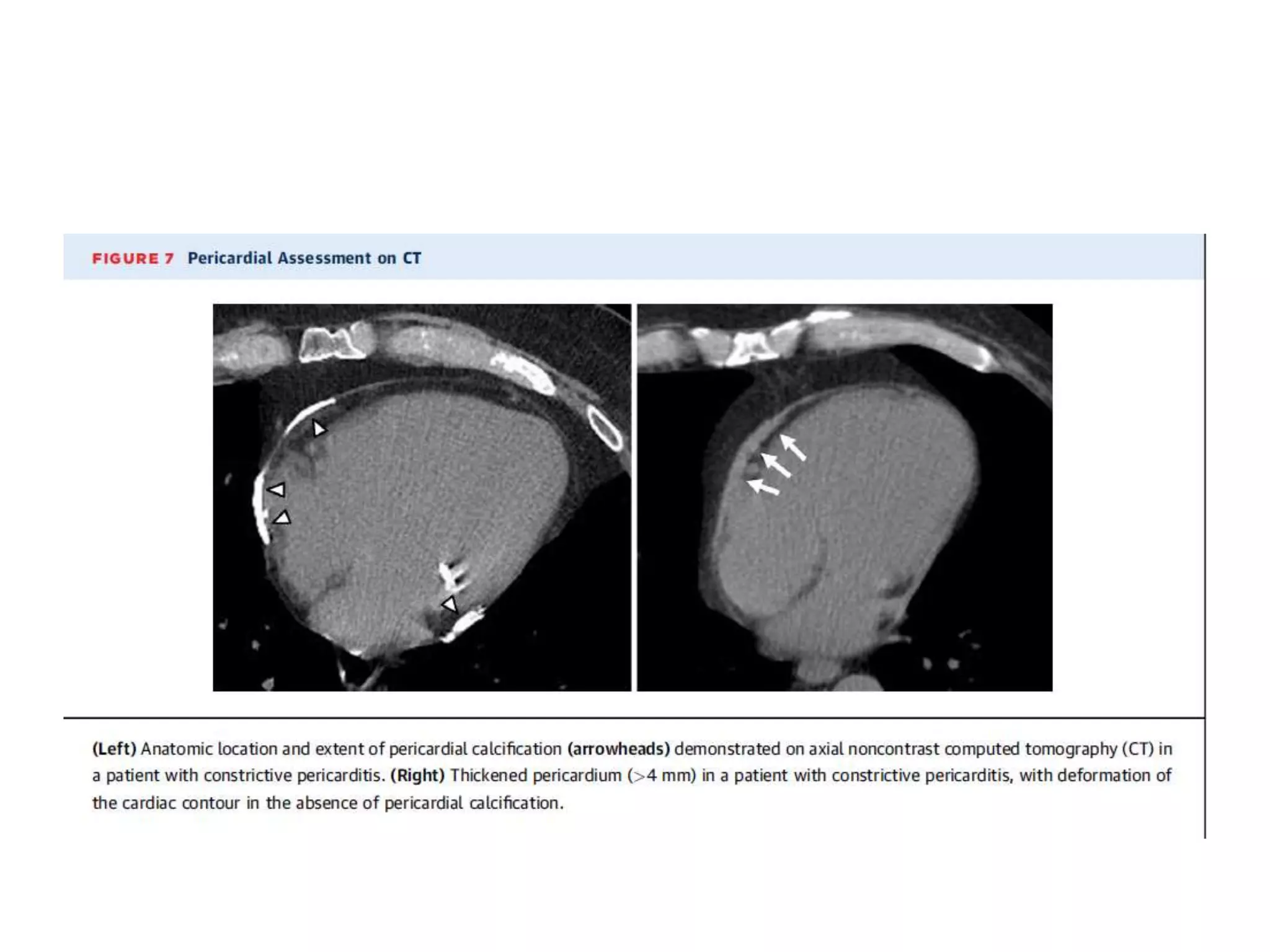











This document discusses the pathophysiology of constrictive pericarditis (CCP). CCP is caused by a thickened and fibrotic pericardium that restricts heart filling. This leads to 4 key hemodynamic changes: 1) impaired diastolic filling, 2) dissociation of intrathoracic and intracardiac pressures with respiration, 3) excessive ventricular coupling, and 4) heart rate dependent filling. The thick pericardium equalizes pressures in all chambers and abruptly halts early diastolic filling. Inspiration decreases left ventricular filling while increasing right ventricular filling via septal shift. Expiration causes the opposite effect.























































































