Primary survey
• A: Can speak, c-spine not tender, full ROM of
neck
• B : Equal breath sound, CCT negative
• C : BP 142/75 mmHg, PR 105 bpm, no active
external bleeding
• D : E4V5M6, pupil 3 mm RTLBE
• E : No external wound, deformity and limit ROM
at left shoulder
6.
Secondary survey
• A: ปฏิเสธประวัติแพ้ยาหรือแพ้อาหาร
• M : ปฏิเสธยาที่ใช้ประจา
• P : ปฏิเสธประวัติโรคประจาตัว
• L : NPO 7.00 น. 21 มกราคม 2560
• E : ผู้ป่ วยล้มจากเตียงแล้วเอามือซ้ายยันพื้นไว้ จากนั้นมี
อาการปวดไหล่ซ้าย รู ้สึกไหล่ซ้ายหลุด ยกแขนซ้ายไม่ได้
ขยับมือได้ เคยไหล่ซ้ายหลุด 2 ครั้งในช่วง 2 เดือนที่ผ่าน
มา
7.
Physical examination
• Generalappearance : A Thai man, alert, well co-
operative
• Vital signs : BP 142/75 mmHg, PR 105 bpm, RR 18
bpm, BT 36.5 ํC
• HEENT : Not pale conjunctivae, anicteric sclera
• Heart : Normal S1S2, no murmur
• Lung : Clear both lungs
• Abdomen : No distension, soft, not tender
• Neurological : Grossly intact
8.
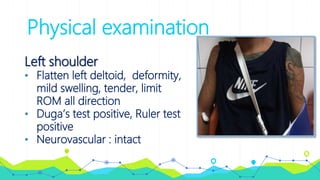
Physical examination
Left shoulder
•Flatten left deltoid, deformity,
mild swelling, tender, limit
ROM all direction
• Duga’s test positive, Ruler test
positive
• Neurovascular : intact
Management
• Pain controlwith MO 5 mg IV stat
• Closed reduction : Traction-countertraction
• On interlocking arm sling
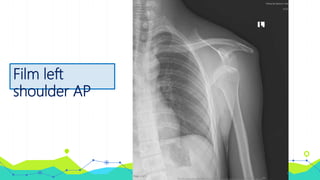
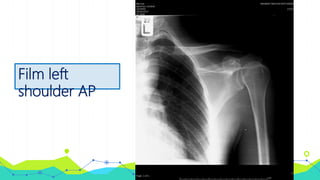
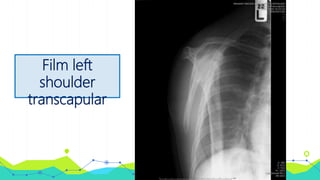
• Film left shoulder AP, left shoulder transcapular หลัง
closed reduction
• Home medication : Paracetamol (500) 1 tab oral prn
for pain q 4-6 hr
• Follow up 2 weeks
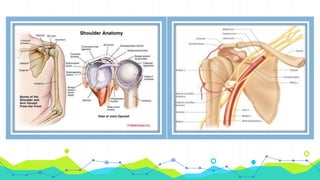
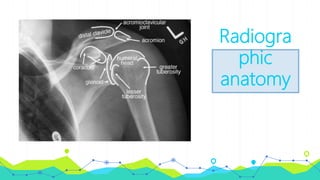
Shoulder (Glenohumeral)
dislocation
• Mostcommonly dislocated joint in the body
• Can occur anteriorly (95-97%), posteriorly (2-
4%), inferiorly, or anterior-superiorly
• Previous shoulder dislocation are more prone
to redislocation
Tissue does not heal properly and/or tissue
stretches out and becomes more lax
Shoulder (Glenohumeral)
dislocation
• Patientswho tear their rotator cuffs or fracture the
glenoid during their shoulder dislocation have a
higher incidence of redislocation
Mechanism of injury
• Anterior dislocation abducted, externally rotated,
extended arm
eg. Blocking a basketball shot, posterior force, fall on
an outstretched arm
• Posterior dislocation adducted, internally rotated
arm
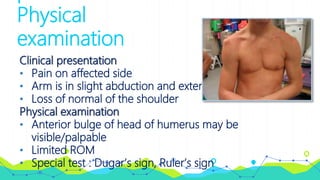
Physical
examination
Clinical presentation
• Painon affected side
• Arm is in slight abduction and external rotation
• Loss of normal of the shoulder
Physical examination
• Anterior bulge of head of humerus may be
visible/palpable
• Limited ROM
• Special test : Dugar’s sign, Ruler’s sign
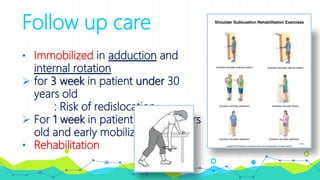
Follow up care
•Immobilized in adduction and
internal rotation
for 3 week in patient under 30
years old
: Risk of redislocation
For 1 week in patient over 30 years
old and early mobilization
• Rehabilitation