Primary Survey atMNRH
• A : Can speak, Full ROM of neck, No C-spine tenderness
• B : Trachea in midline, Equal breath sound, RR 20/min,
Chest compression test negative
• C : BP 125/89 mmHg, PR 82 bpm, Pelvic compression test negative
• D : E4V5M6, Pupil 2 mm RTLBE
• E : Laceration wound 3 x 1 cm at dorsum of right foot, No deformity,
No active bleeding
6.
Secondary Survey
• A: No history of food and drug allergy
• M : No current medication
• P : No underlying disease
• L : Last meal 1 hour before go to hospital
• E : As present illness
7.
Present Illness
2 ชั่วโมงก่อนมาโรงพยาบาลหลังดื่มสุราเสร็จ(ประมาณ 19.00 น.) ได้ขับรถกลับบ้าน ระหว่างทางผู้ป่วย
ขับรถตกหลุมบนถนนเสียหลักล้ม อะไหล่รถที่เป็นเหล็กทิ่มเท้าขวา มีแผลเปิดเลือดไหลที่หลังเท้าขวา ปวดมาก
พอเดินได้ขยับข้อเท้าและนิ้วเท้าได้ไม่มีแผลหรือเจ็บบริเวณอื่น
Past history
- ปฎิเสธประวัติโรคประจาตัว/ประวัติผ่าตัด
- ปฏิเสธประวัติอุบัติเหตุรุนแรงอื่นๆ
Physical Examination
• V/S: Temp 36 c, BP 125/89 mmHg, HR 82 bpm, RR 14 /min
• GA : A Thai man, Good consciousness
• HEENT : No pale conjunctivae, Anicteric sclerae
• Neck : Active movement
• Heart : Normal S1 S2 no murmur
• Respiratory : Normal breath sound, Equal both lung
• Abdomen : Soft, not tender, Normoactive bowel sound
10.
Physical Examination
• Extremities: Rt. Foot - Laceration wound size 3 x 1 cm. at lateral side
in dorsum of foot, No active bleeding,
no fat globule seen, no deformity
- Motor : Limit due to pain but can
dorsi/plantar flexion, eversion and
inversion
- Sensory : intact
- Capillary refill : 2+
: Others - WNL
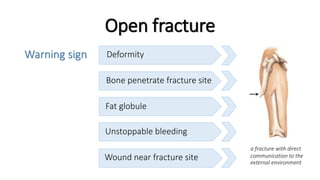
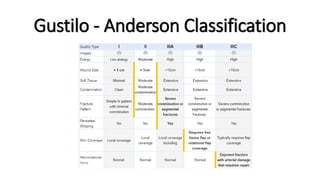
Warning sign
Open fracture
Deformity
Bonepenetrate fracture site
Fat globule
Unstoppable bleeding
Wound near fracture site
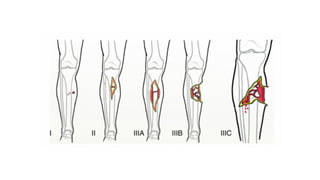
a fracture with direct
communication to the
external environment
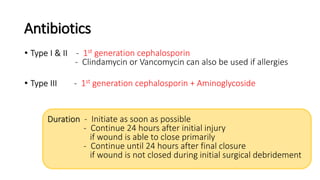
Antibiotics
• Type I& II - 1st generation cephalosporin
- Clindamycin or Vancomycin can also be used if allergies
• Type III - 1st generation cephalosporin + Aminoglycoside
Duration - Initiate as soon as possible
- Continue 24 hours after initial injury
if wound is able to close primarily
- Continue until 24 hours after final closure
if wound is not closed during initial surgical debridement
Stabilization
• Splint fracturefor temporary stabilization
• Assess soft tissue damage and neurovascular injury
decreases pain,
further injury from bone ends,
and disruption of clots
22.
Basic Principles ofOpen Fracture
Management in the Operating Room
• When ?
- as soon as possible ( emergency )
• How ?
- Debridement
- Irrigation
- Fracture stabilization
- Wound closure
23.
Basic Principles ofOpen Fracture
Management in the Operating Room
• Aggressive debridement and irrigation
- Thorough debridement is critical to prevention of deep infection
- Low and high pressure lavage are equally effective in reducing
bacterial counts
- Saline shown to be most effective irrigating agent
- Bony fragments without soft tissue attachment can be removed
Type I – 3 L Type II – 6 L Type III – 9 L
24.
Basic Principles ofOpen Fracture
Management in the Operating Room
• Fracture stabilization
- can be with internal or external fixation, as indicated
• Staged debridement and irrigation
- performed every 24 or 48 hours as needed
• Early soft tissue coverage or wound closure is ideal
- increased risk of infection beyond 7 days
25.
Basic Principles ofOpen Fracture
Management in the Operating Room
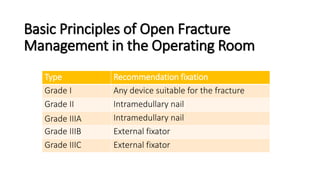
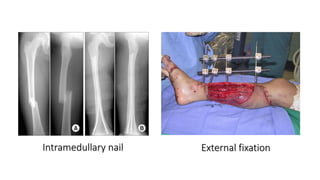
Type Recommendation fixation
Grade I Any device suitable for the fracture
Grade II Intramedullary nail
Grade IIIA Intramedullary nail
Grade IIIB External fixator
Grade IIIC External fixator