Recommended
PPTX
Extern conference orthopedics Ext.กิตตินันทน์ 12 กพ.61
PPTX
Conference ant shoulder dislocation
PPTX
PDF
PPT
ATLS- Advanced Trauma Life Support
PDF
Case conference ortho pdf
PPTX
PDF
Open fracture wound care_Dr anglen
PPTX
Ac dislocation dangtoandhy
PDF
Proximal femoral fractures
PPTX
Supracondylar humeral fracture
PDF
Management of Geriatric Distal Radius Fracture: Now and Then
PDF
PPTX
Paediatric forearm fractures
PPTX
PPTX
Extern conference.thitirat
PDF
PPTX
Clinical practice guidelines mild head injury
PPTX
PPTX
Damage Control Orthopaedics (DCO)
PPTX
PDF
PATIENT ASSESSMENT GENERAL FORM
PDF
Emergency care to head injured patient
PPTX
PPTX
Fractures around the knee
PPT
PPT
PDF
Distally-Based Sural Flap
PPTX
Case conference ศุภกิตติ์
PPTX
Extern orthopedic-conference-prima
More Related Content
PPTX
Extern conference orthopedics Ext.กิตตินันทน์ 12 กพ.61
PPTX
Conference ant shoulder dislocation
PPTX
PDF
PPT
ATLS- Advanced Trauma Life Support
PDF
Case conference ortho pdf
PPTX
PDF
Open fracture wound care_Dr anglen
What's hot
PPTX
Ac dislocation dangtoandhy
PDF
Proximal femoral fractures
PPTX
Supracondylar humeral fracture
PDF
Management of Geriatric Distal Radius Fracture: Now and Then
PDF
PPTX
Paediatric forearm fractures
PPTX
PPTX
Extern conference.thitirat
PDF
PPTX
Clinical practice guidelines mild head injury
PPTX
PPTX
Damage Control Orthopaedics (DCO)
PPTX
PDF
PATIENT ASSESSMENT GENERAL FORM
PDF
Emergency care to head injured patient
PPTX
PPTX
Fractures around the knee
PPT
PPT
PDF
Distally-Based Sural Flap
Similar to Ortho conference - anterior shoulder dislocation
PPTX
Case conference ศุภกิตติ์
PPTX
Extern orthopedic-conference-prima
PPTX
Case conference shoulder dislocation
PPTX
PPTX
Extern orthopedic-conference-prima
PPTX
Extern conference : Fracture mid shaft humerus
PPTX
Extern conference-สรรเสริญ ศรีสุวัจฉรีย์
PPTX
PDF
PPTX
Conference ext.อิศรา เย็นยุวดี (เต้ย รพ.รามา)
PPTX
colles' fracture case dicussion
PDF
PPTX
Morning conference ortho ดรีม
PPTX
Ext conference Ext.ภัทรานิษฐ์ ชัยติวร 27 พ.ย. 60
PPTX
distal end radius fracture
PDF
PPTX
Anterior shoulder-dislocation
PPTX
PPTX
PPTX
Fracture distal end radius
Ortho conference - anterior shoulder dislocation 1. 2. 3. • 14 ชั่วโมงก่อนมารพ. สะดุดล้มเอง แขน
ซ้ายกระแทกพื้น ปวดบวมบริเวณไหล่ซ้าย ไม่
มีแผลเปิด ขยับแขนซ้ายไม่ไหวเพราะรู้สึกเจ็บ
ไม่มีอาการชาหรืออ่อนแรง ไม่มีศีรษะ
กระแทกพื้น ไม่สลบ จาเหตุการณ์ได้
Present illness :
4. • มีประวัติ ล้ม แล้วไหปลาร้าข้างซ้ายหัก
• ปฏิเสธประวัติเคยได้รับการผ่าตัด
• ปฏิเสธประวัติโรคประจาตัว
• ปฏิเสธประวัติแพ้ยาแพ้อาหาร
• ไม่มีประวัติทานยาเป็นประจา
Past history :
5. Physical examination :
• Vital signs – T 36.5 c , PR 94 bpm , BP 130/92 mmHg , RR 20 /min
• GA - A Thai elderly man , alert , good consciousness
• HEENT – no pale conjunctivae , anicteric sclarae
• CVS – regular and symmetrical pulses all extremities , normal s1s2 , no
murmur , capillary refill < 2 sec
• Lungs – no dypsnea , normal and equal breath sound on both lungs ,
no adventitious sound
• Abdomen – normoactive bowel sound , soft , not tender
6. Physical examination :
Extremities ( Left shoulder ) –
Ruler’s and Duga’s sign positive ,
tender and swelling around left
shoulder joint , radial pulse 2+ ,
axillary nerve intact , limit ROM
due to pain
7. 8. 9. 10. history :
Refer จาก รพช.
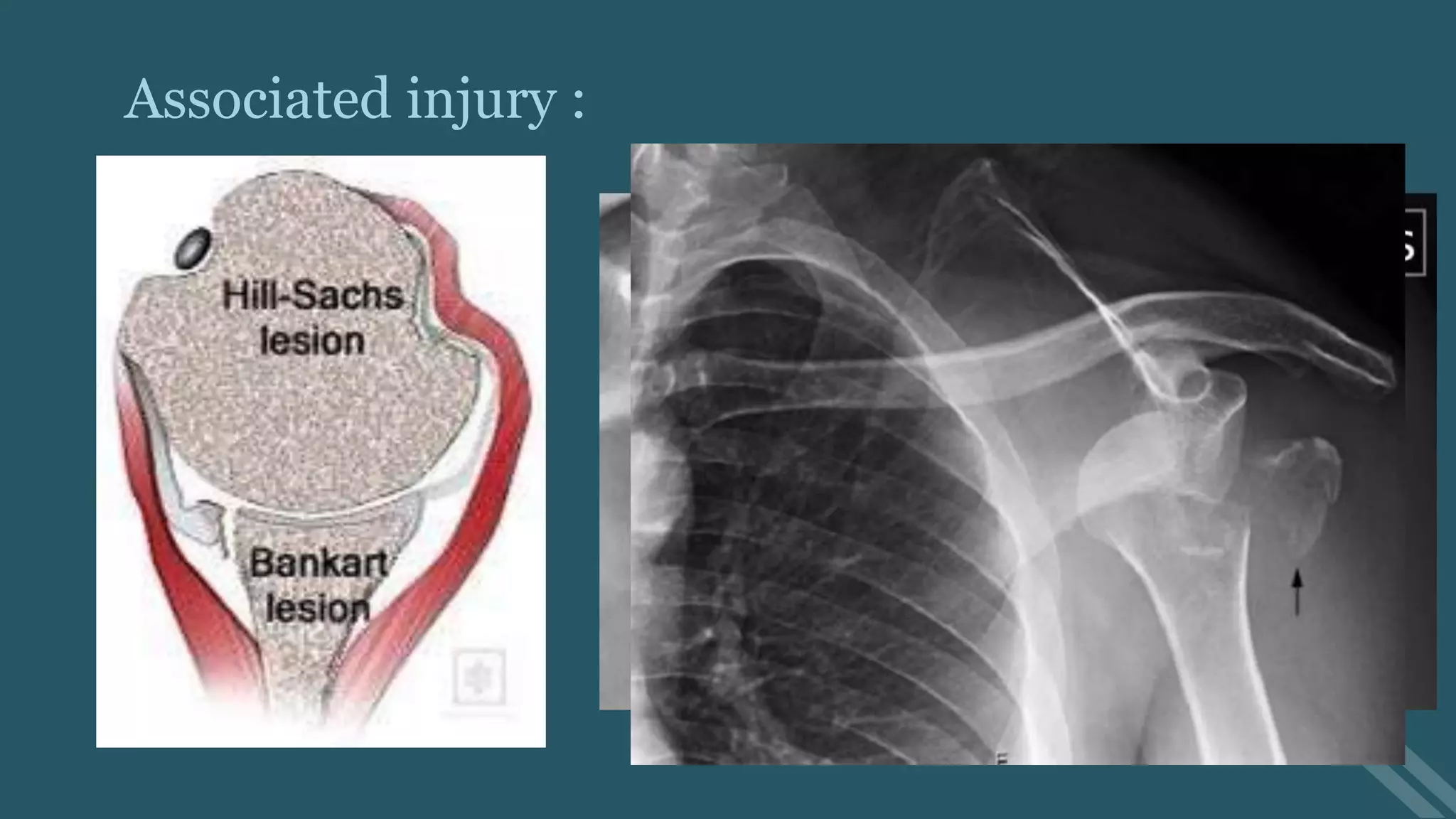
film : Anterior left shoulder dislocation
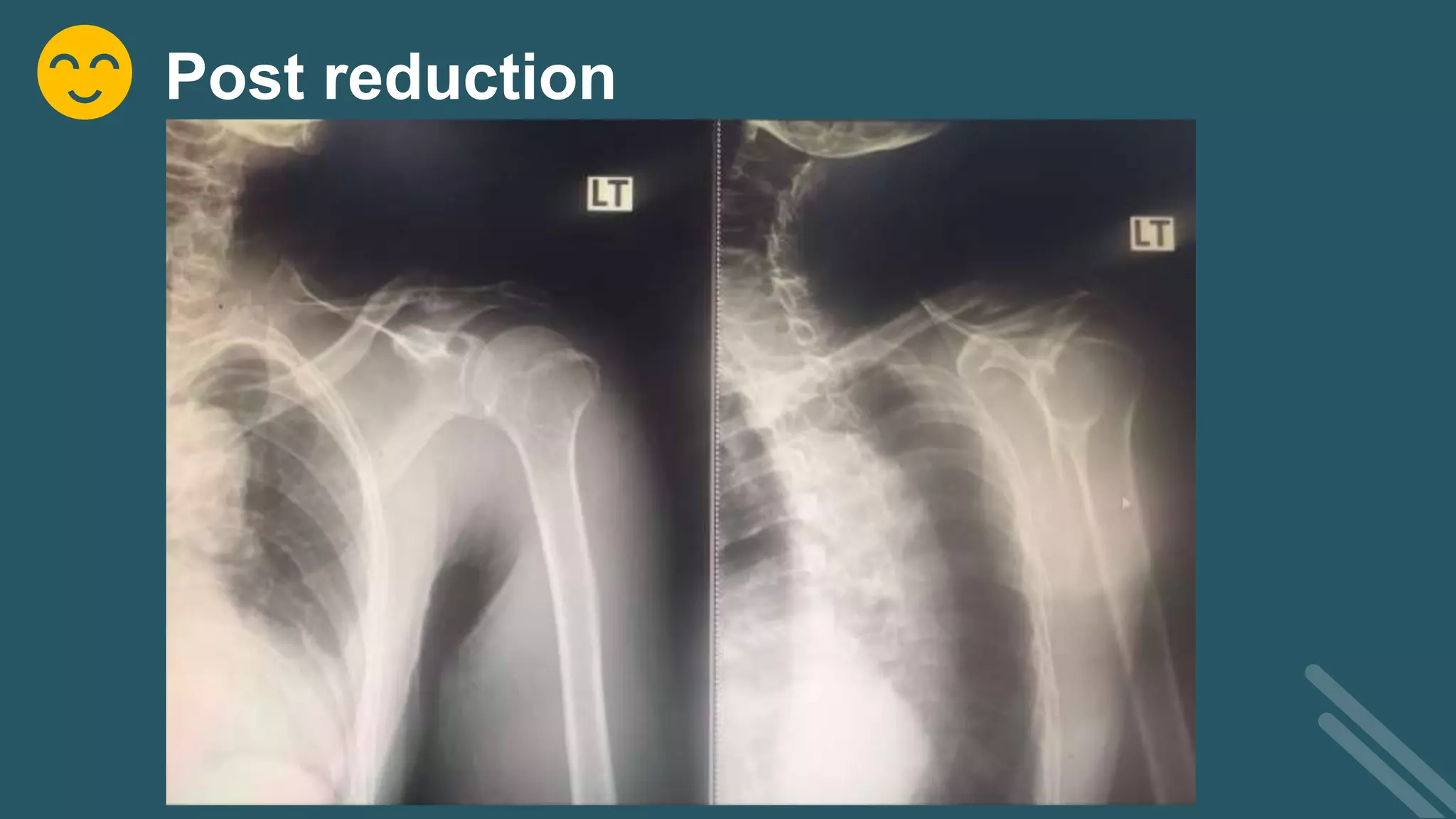
Management : MO 5 mg IV stat ,
Valium 5 mg IV stat —> closed
reduction —> fail
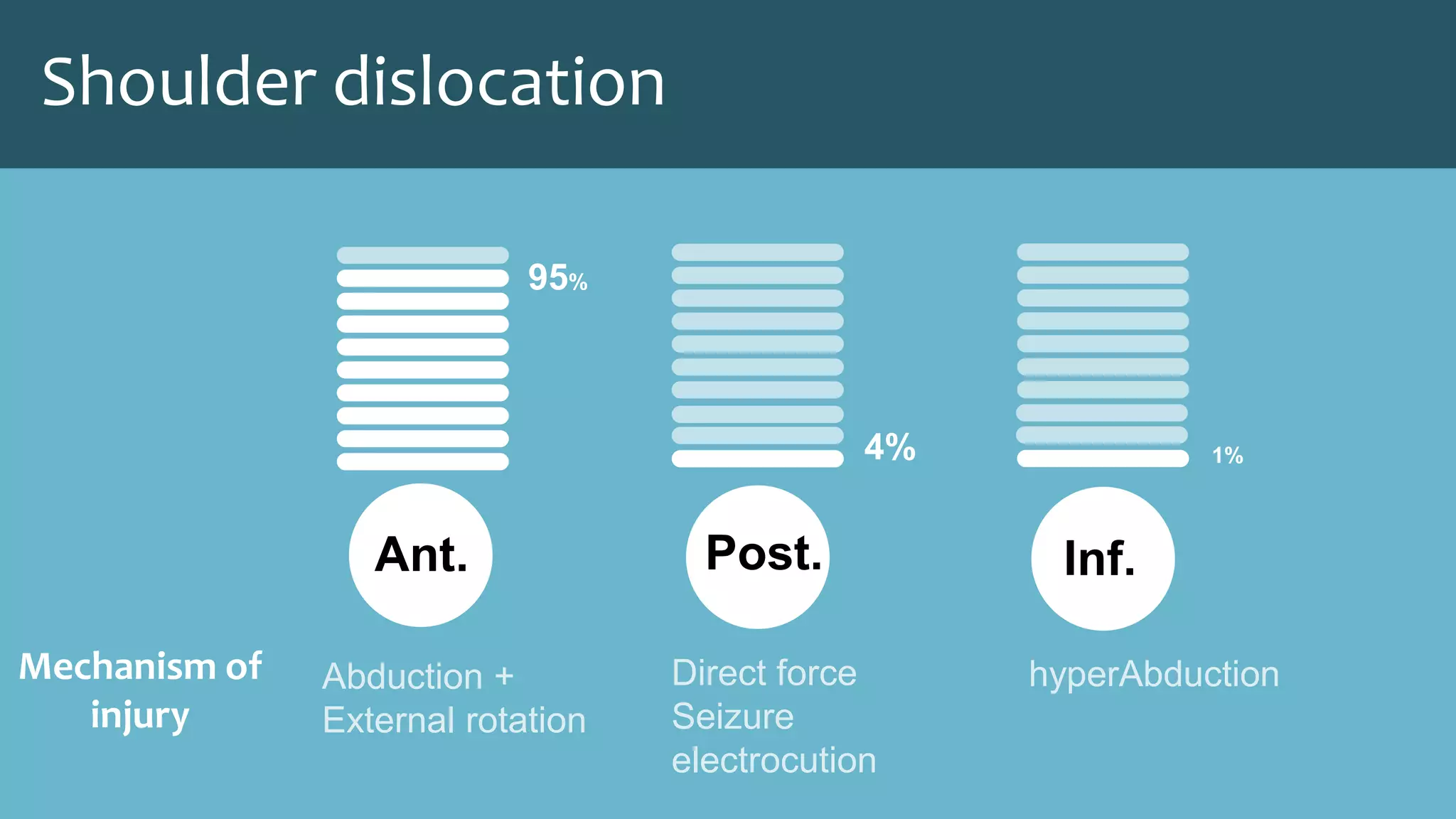
11. 12. 13. 14. sign & symptom :
• Shoulder pain
• Abduction and external
rotation position
• Ruler sign
• Duga sign
• Axillary nerve injury :
impaired sensation of
deltoid area, deltoid muscle
weakness
Plain film x-ray :
• AP view
• Transcapular view
• Transaxillary view
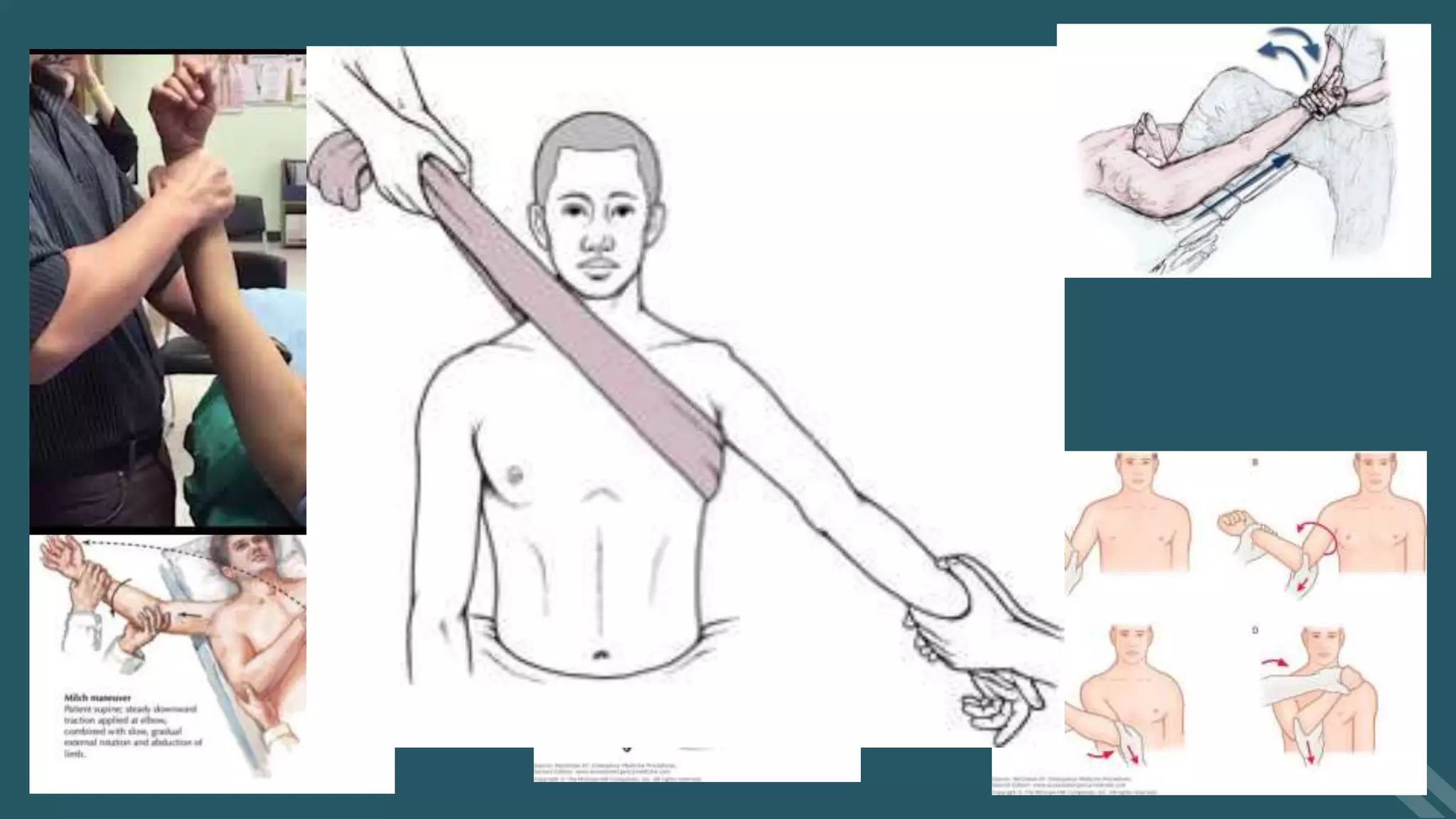
15. 16. 17. Management :
Analgesia & Sedation
Reduction
• Zero position
• Traction counter traction
• Stimson technique
• Kocher’s technique
19. 20. 21. 22.