Downloaded 658 times
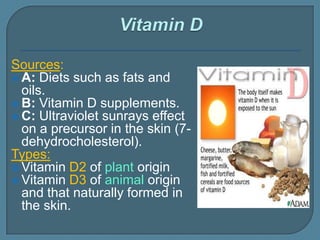
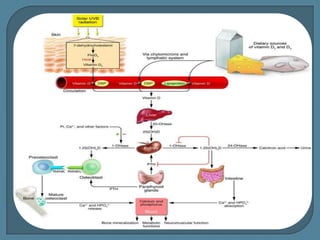
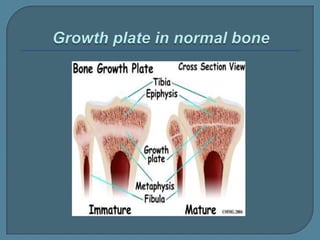
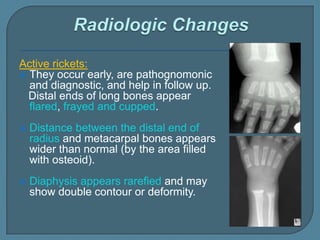
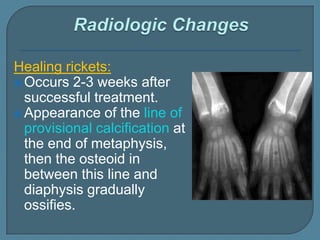

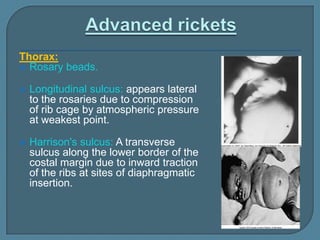
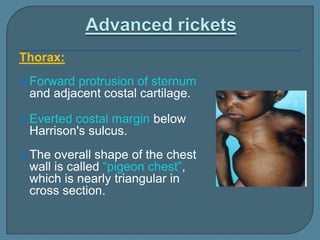
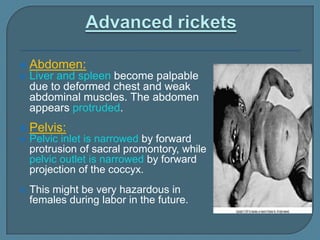
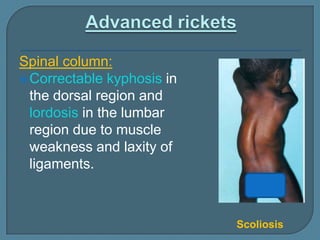
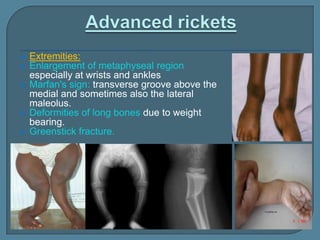



This document discusses rickets, a disease characterized by defective bone mineralization due to vitamin D deficiency or abnormal metabolism. It covers the sources and types of vitamin D, how vitamin D is metabolized in the body, and its actions in increasing calcium and phosphate absorption and bone mineralization. Symptoms of rickets are described including bone deformities, craniotabes, and rosary beads. Diagnosis involves physical exam findings, elevated alkaline phosphatase levels, and x-rays showing metaphyseal changes. Treatment is aimed at correcting the vitamin D deficiency through sunlight exposure or vitamin D supplementation. Prognosis is generally good with treatment but deformities may require orthopedic correction.























































































