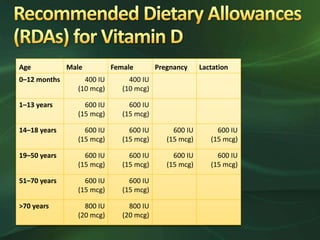
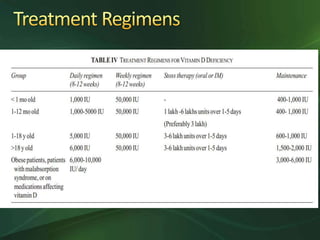
The document outlines vitamin D intake recommendations for various age groups, emphasizing the higher needs during pregnancy and lactation, especially for certain populations like those with obesity or on specific medications. It also discusses treatment for vitamin D deficiency and the importance of calcium supplementation during therapy. Recommendations include administering high doses of vitamin D to breastfeeding mothers and fortifying food to ensure adequate intake.