Downloaded 306 times

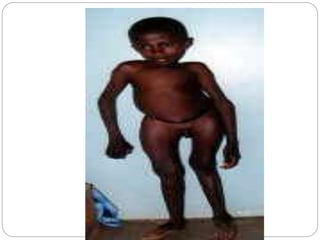

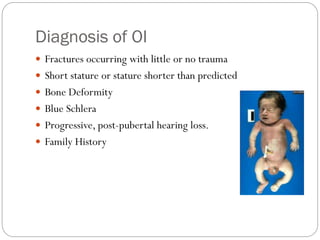
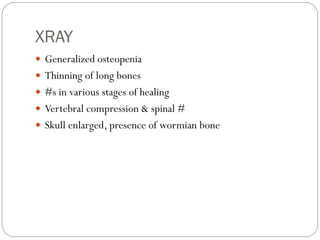





Osteogenesis imperfecta, or brittle bone disease, is caused by mutations in collagen genes COL1A1 and COL1A2 that result in abnormal bone formation and fragility. It is characterized by bones that break easily from minor trauma, along with other connective tissue problems like blue sclera and joint laxity. Treatment focuses on preventing fractures through braces and limiting activity, as well as bisphosphonates and surgery to insert rods for stabilization. The disease ranges in severity from mild cases with normal life expectancy to lethal prenatal forms.





























































































