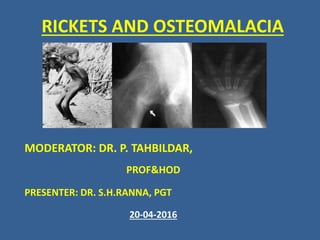
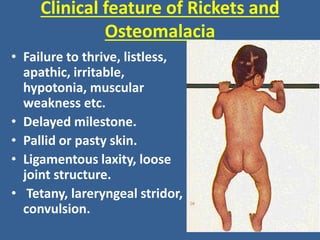
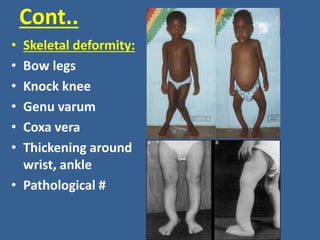
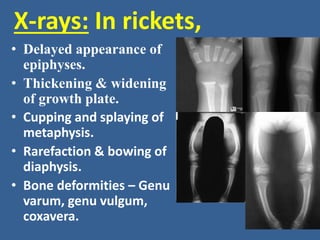
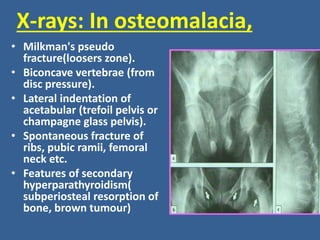
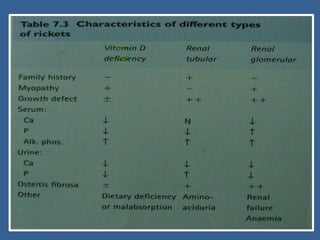
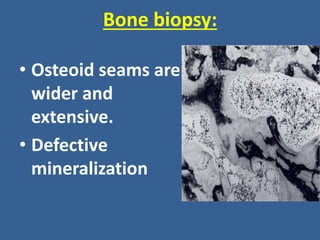
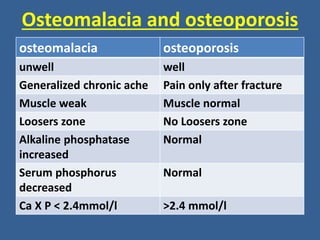
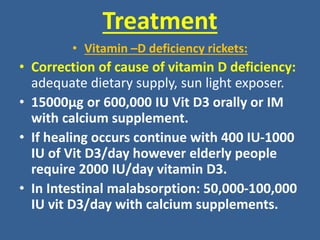
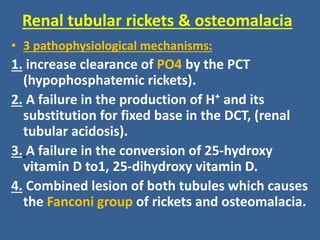
Rickets and osteomalacia are diseases caused by inadequate bone mineralization due to vitamin D deficiency or impaired mineral metabolism. Rickets primarily affects children as it involves the growth plates, while osteomalacia affects adults. Symptoms include bone pain, deformities, and fractures. Diagnosis involves blood tests showing low calcium and phosphate levels and high alkaline phosphatase. X-rays show abnormalities in bone structure and density. Treatment focuses on correcting the underlying causes through vitamin D and calcium supplementation, with surgical intervention for severe deformities.