Downloaded 419 times










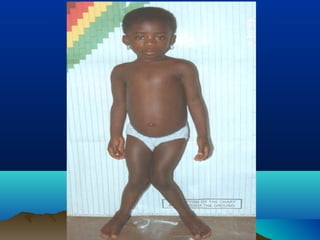
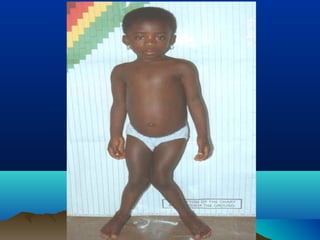


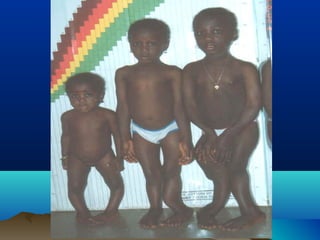
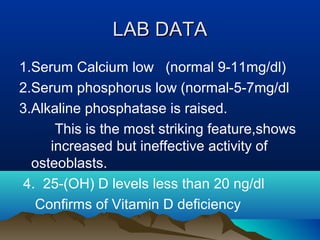
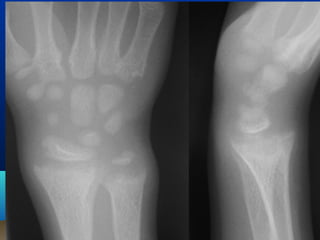



This document discusses rickets, a disease caused by vitamin D deficiency or impaired mineralization that affects growing bones in children. It defines rickets and outlines various types including nutritional, vitamin D dependent, and vitamin D resistant rickets. Clinical features like softening of bones and skeletal deformities are described. Laboratory findings of low calcium and phosphorus and high alkaline phosphatase are also summarized. The document outlines prevention through diet, supplementation, and sunlight exposure as well as treatment with high dose vitamin D or calcium therapy.























































































