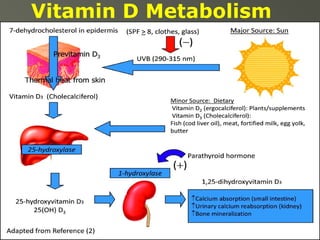
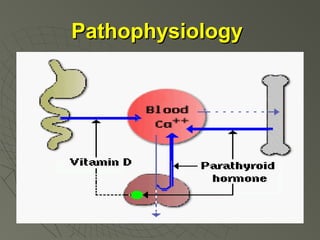
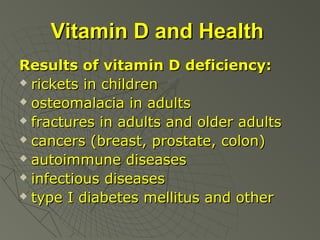
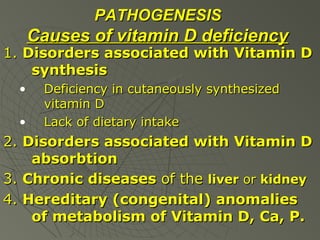
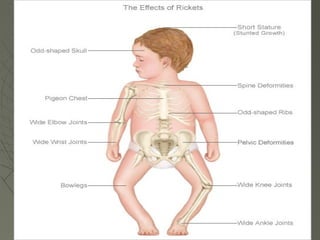
This document provides an overview of rickets presented by Lyudmyla Olexandrivna Rakovska from the Department of Pediatrics at V.N. Karazin Kharkiv National University. The 10-point plan discusses the definition, etiology, pathogenesis, classification, clinical manifestations, laboratory/radiological findings, differential diagnosis, treatment and prevention of rickets. Key points include that rickets is caused by vitamin D deficiency impairing bone mineralization, especially in children under 2 years old. Symptoms involve soft, deformed bones and skeletal abnormalities. Treatment focuses on vitamin D supplementation through either low daily doses or high single doses.






























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)










