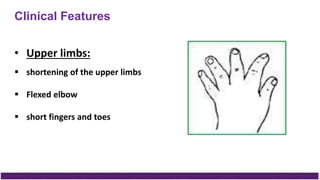
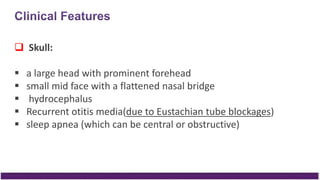
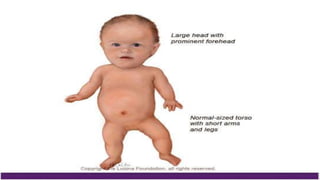
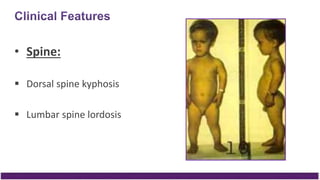
Achondroplasia is a genetic disorder characterized by disproportionate short stature and limb abnormalities. It results from a mutation on chromosome 4 that causes a defect in bone growth by disrupting endochondral ossification. Individuals with achondroplasia have short stature, an enlarged head, midface hypoplasia, spinal abnormalities, and shortened limbs disproportionately affecting the arms and thighs. Complications can include neurological problems, respiratory issues, and spinal stenosis. While there is no cure, treatment focuses on supportive care, surgery to address orthopedic issues, and in some cases growth hormone therapy.






![A lumbar spine (anteroposterior [AP]) view
reveals distinct narrowing on the interpedicular
distances from proximal to distal (see the
image).
Normally, the interpedicular distance from the
cephalocaudad direction should increase.](https://image.slidesharecdn.com/8888-171231200314/85/Achondroplasia-19-320.jpg)





























































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)







