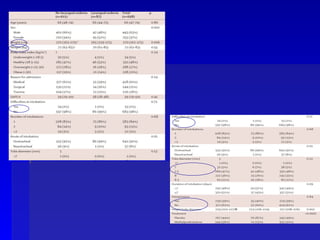
The document discusses post-extubation stridor, which is upper airway obstruction that can occur after a patient is extubated from a ventilator. It defines post-extubation stridor and reviews risk factors such as duration of intubation and cuff pressures. The cuff leak test is presented as a way to identify patients at risk. Studies are reviewed showing steroids given before extubation can reduce the risk of stridor. Clinically, it recommends identifying at-risk patients, performing the cuff leak test, and considering steroid treatment for high-risk patients before extubation.