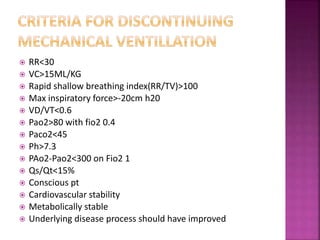
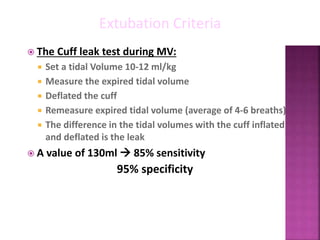
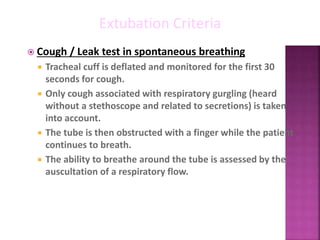
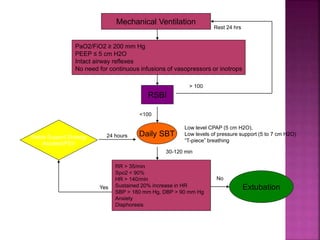
The document discusses various methods for weaning patients off mechanical ventilation, including SIMV, T-piece trials, CPAP/BiPAP, and pressure support. It notes major factors to consider for each patient such as their primary illness, ventilatory support needs, and other medical conditions. Key criteria for determining readiness for weaning trials and extubation include respiratory rate, vital capacity, gas exchange values, hemodynamic stability, and underlying disease improvement. Factors that could lead to weaning or extubation failure are also outlined.