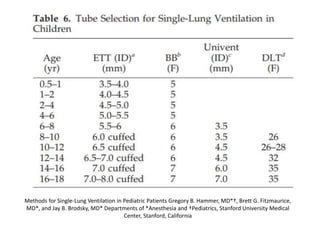
This document discusses options for lung isolation during surgery, including double lumen tubes (DLTs) and bronchial blockers. It provides details on:
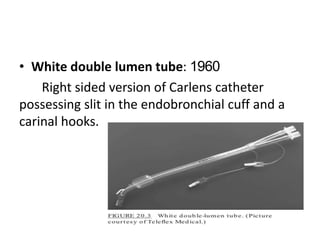
1) The history and development of DLTs from the 1950s onward, including specific DLT designs like the Carlens tube.
2) Guidance on proper DLT placement using bronchoscopy to position the endobronchial cuff below the carina in the left or right bronchus.
3) Both advantages and disadvantages of DLTs and bronchial blockers for lung isolation are outlined. Positioning DLTs requires bronchoscopy while blockers can be placed through a standard endotracheal tube but dislodge