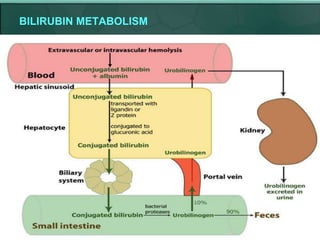
This document discusses obstructive jaundice, providing definitions, pathophysiology, effects on various body systems, etiology, history and examination findings, laboratory investigations, imaging modalities, and causes of biliary obstruction. It defines obstructive jaundice as a failure of bile to reach the intestine due to mechanical obstruction. Pathophysiological changes include bile duct dilation, hepatic fibrosis, and portal hypertension. Causes include gallstones, strictures, tumors, and congenital anomalies. A thorough history, physical exam, and lab tests can localize the level and cause of obstruction, while imaging modalities like ultrasound and MRCP can identify and characterize obstructive lesions.

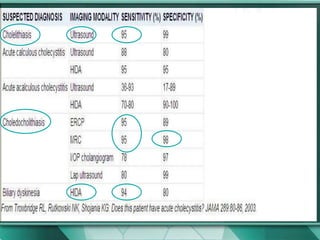
![Ultrasonography
Ultrasound of the abdomen is an extremely useful and accurate method for
identifying gallstones and pathologic changes in the gallbladder consistent with
acute cholecystitis. Abdominal ultrasound, if performed by an experienced
operator, should be part of the routine evaluation of patients suspected of having
gallstone disease, given the high specificity (>98%) and sensitivity (>95%) of this
test for the diagnosis of cholelithiasis[1] ( Table 54-1 ). In addition to identifying
gallstones, ultrasound can also detail signs of cholecystitis such as thickening of
the gallbladder wall, pericholecystic fluid, and impacted stone in the neck of the
gallbladder. It is often the initial screening test for patients with suspected
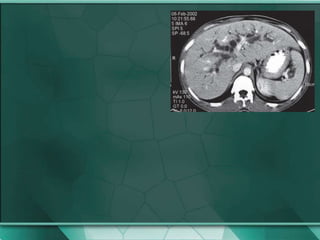
extrahepatic biliary obstruction ( Fig. 54-7 ). Dilation of the extrahepatic (>10 mm)
or intrahepatic (>4 mm) bile ducts suggests biliary obstruction. Intraoperative
ultrasound is now used frequently to further evaluate intrahepatic lesions, assess
resectability, and determine involvement of vascular structures](https://image.slidesharecdn.com/obstructivejaundice-kk-101027013911-phpapp01/85/Obstructive-jaundice-41-320.jpg)