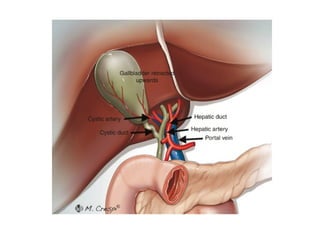
Porta hepatis
Relationof structures at the porta
hepatis from before backwards are: „
Hepatic ducts in the front „
Branches of hepatic artery „
Branches of portal vein.
7.
Blood supply
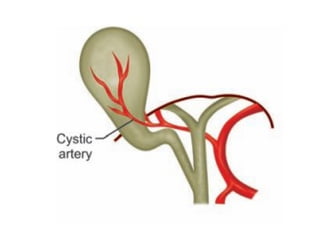
Gallbladderis supplied by the cystic
artery which is usually a branch of right
hepatic artery.
Bile duct is supplied by two vertical
arteries arising from the hepatic artery
running along the bile duct at 3 and 9
o’clock position and giving of
circumferential arteries anteriorly and
posteriorly.
11.
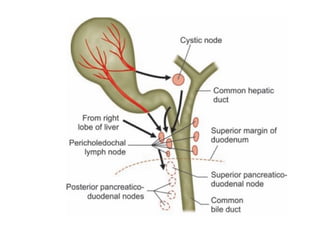
Lymphatic supply
Lymphaticsof gallbladder drain into the
cystic lymph node of Lund.
Efferent from the cystic lymph nodes
drains into the pericholedochal lymph
nodes and lymph nodes at the porta
hepatis and supeorior and posterior
pancreatico dudenal lymph nodos.
These lymphatic then passes into the
celiac lymph nodes
Definition
It isthe jaundice that develops due to
biliary obstruction, partial or complete
or intermittent.
It causes conjugated
hyperbilirubinaemia.
Normal serum bilirubin level is 0.2-0.8
mg%.
Scleral icterus is visible when serum
bilirubin level exceeds 2.5 mg%.
15.
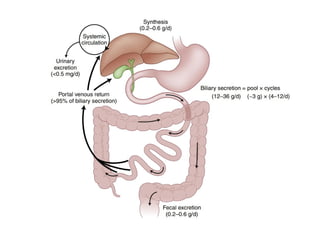
Bilirubin metabolism and
enterohepaticcirculation
Aged red cells get lysed in the
reticuloendothelial cells and breakdown
into haem and globin.
Bilirubin is combined with albumin
and transported to liver.
In the liver bilirubin get separated from
albumin and conjugated to bilirubin
glucuronide by glucuronyl
transferase.
16.
This conjugatedbilirubin glucuronide is
water soluble and can be excreted in
kidney (So in obstructive and hepatic
jaundice bile pigment - bilirubin is seen
in the urine).
This conjugated bilirubin is excreted
through biliary canaliculi reaching
intestine.
In the intestine, it is converted into
stercobilinogen and urobilinogen by
17.
70% ofthis is absorbed in the colon and
brought back to liver as enterohepatic
circulation.
Unabsorbed stercobilinogen colours
faeces brown.
Circulating urobilinogen is taken up by
kidneys for excretion.
18.
Normal urinaryurobilinogen is 100-200
mg/day. It is absent in obstructive
jaundice.
Normal faecal stercobilinogen is 300
mg/day. It is also absent in obstructive
jaundice.
20.
Pathophysiology in obstructive
jaundice
Obstructive jaundice, often called as surgical
jaundice occurs due to intrahepatic or
extrahepatic biliary outflow obstruction.
It leads into cholestasis which means
conjugated hyperbilirubinaemia; probably
due to impaired bile flow and impaired bile
formation.
Bile acid secretion into the gut is impaired
causing defective absorption of fat and
fat-soluble vitamins like vitamin K;
21.
this, in turncauses poor synthesis of
prothrombin and conversion of
prothrombin to thrombin causing widened
PT and PT INR.
Factors II, VII, IX, and X are vitamin K-
dependent clotting factors.
PT indicates the extrinsic pathway of
coagulation; whereas partial thromboplastin
time represents the intrinsic pathway.
Bile acid stasis causes hepatocytes injury.
22.
Fat malabsorptioncauses steatorrhoea and
also deficiencies of vitamins A (visual
problem, thick skin), D (osteomalacia), E
(peripheral neuropathy, cerebellar ataxia,
posterior column dysfunction), K (bleeding
tendencies).
Persistent cholestasis may be associated
with deposits of cholesterol in the skin
(cutaneous xanthomatosis), occasionally in
bones and peripheral nerves.
23.
Bilirubinostasis (bileplugs) cause
hepatocytes degeneration, small duct and
ductular obstruction, pericholangitis,
oedema, bile leak, liver infarction and biliary
cirrhosis.
Obstruction may be due to benign conditions
like biliary tree stones (most common cause)
or strictures or sclerosing cholangitis; or
due to malignant conditions like carcinoma
of pancreas or cholangiocarcinoma.
24.
Extrahepatic obstructionmay be
Luminal (stones, infestations [ascariasis,
clonorchis sinensis and schistosomiasis) or
Mucosal/wall (growth, stricture [post-
inflammatory, postsurgical or post-RT],,
primary sclerosing cholangitis) or
External compression (pancreatitis,
pancreatic tumour, compression by
nodal mass).
25.
lntrahepatic cholestasisgenerally occurs at
the level of the hepatocyte or biliary
canalicular membrane. Causes include
hepatocellular disease (e.g. viral hepatitis,
hepatitis/cholestasis (thiazides,
chlorpromazine), biliary cirrhosis.
In hepatocellular disease, interference in
the 3 major steps of bilirubin metabolism-
uptake, conjugation and excretion usually
occur.
26.
The lackof bilirubin in the intestinal
tract is responsible for the pale stools in
biliary obstruction.
The cause of itching (pruritus)
associated with biliary obstruction is
related to the accumulation of bile acids
in the skin.
27.
Severe biliaryobstruction causes cell
damage usually in 1 month and, if
unrelieved, may lead to secondary
biliary cirrhosis.
Acute cholangitis is another
complication associated with
obstruction of the biliary tract and is
the most commonly seen in stricture,
most often at the level of the CBD.
28.
Bile flowobstruction stasis
colonization and multiplication of
bacteria concomitant increased
intraductal pressure reflux of biliary
contents bacteremia, septicaemia
septic shock.
29.
Effects of Obstructive
Jaundice
In liver. Enlarged green bile stained liver
(hydrohepatosis) shows dilated
intrahepatic biliary radicles.
Once intraductal CBD pressure
increases bile secretion from liver is
reduced causing formation of 'white
bile' in CBD.
Biliary cirrhosis may develop later.
In the biliary tree: Recurrent
inflammation-cholangitis, fibrosis can
30.
In bowel:Absence of bile from bowel
impairs digestion, reduces fat
absorption making faeces bulky and
fatty.
Vitamin K absorption is reduced
causing fall in prothrombin level
raising PT-INR.
Retention of bile salts and bile
pigments in blood and body fluids
occurs.
31.
Classification of Causesof
Obstructive Jaundice
1. Congenital: Biliary atresia, choledochal cyst.
2.Inflammatory: Ascending cholangitis,
sclerosing cholangitis.
3.Obstructive: CBD stones, biliary stricture,
parasitic infestation.
4.Neoplastic: Carcinoma of head or
periampullary region of pancreas,
cholangiocarcinomas, Klatskin tumour.
5.Extrinsic compression of CBD by lymph
nodes or tumours.
33.
Clinical features
Severejaundice.
Pruritus, more on the back and forearms.
Fever, may or may not be present.
Loss of weight.
Loss of appetite.
Pain in right hypochondrium,
Palpable gallbladder.
Hydrohepatotic palpable, smooth, soft,
non-tender liver.
34.
Courvoisier's lawmay suggest
inflammatory/neoplastic cause.
Charcot's triad/Reynold's pentad as
presentation in cholangitis.
Steatorrhoea (more fatty stool) due to
improper absorption of fat soluble
vitamins.
35.
Courvoisier’s law
Ifin a jaundice patient, the gallbladder is
palpable, then it is not due to
choledocholithiasis as the gallbladder would
have been "brosed by previous cholecystitis.
Exceptions „
Double impaction of stone—one at common
bile duct and another at cystic duct „
Primary CBD stone „
Distended gallbladder due to large stone
load.
36.
Clinical assessment of
jaundice
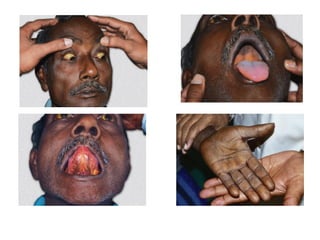
Jaundice is defined as yellowish
discoloration of skin, eyes and mucous
membrane due to excessive bilirubin in
blood.
Jaundice is looked for in upper bulbar
sclera, soft palate, undersurface of tongue,
palms, soles and general body skin.
Clinical jaundice is seen when the bilirubin
level is more than 2 mg%.
38.
Investigations for Obstructive
Jaundice
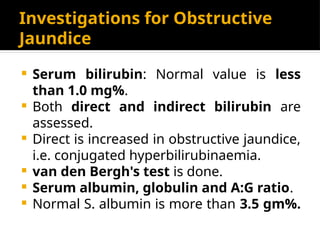
Serum bilirubin: Normal value is less
than 1.0 mg%.
Both direct and indirect bilirubin are
assessed.
Direct is increased in obstructive jaundice,
i.e. conjugated hyperbilirubinaemia.
van den Bergh's test is done.
Serum albumin, globulin and A:G ratio.
Normal S. albumin is more than 3.5 gm%.
39.
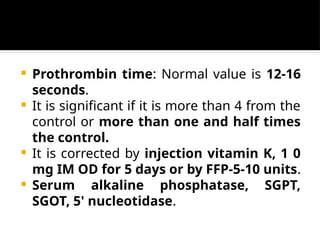
Prothrombin time:Normal value is 12-16
seconds.
It is significant if it is more than 4 from the
control or more than one and half times
the control.
It is corrected by injection vitamin K, 1 0
mg IM OD for 5 days or by FFP-5-10 units.
Serum alkaline phosphatase, SGPT,
SGOT, 5' nucleotidase.
40.
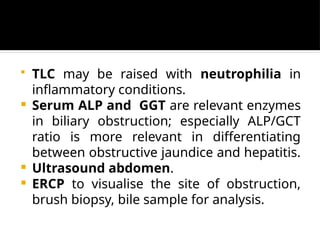
TLC maybe raised with neutrophilia in
inflammatory conditions.
Serum ALP and GGT are relevant enzymes
in biliary obstruction; especially ALP/GCT
ratio is more relevant in differentiating
between obstructive jaundice and hepatitis.
Ultrasound abdomen.
ERCP to visualise the site of obstruction,
brush biopsy, bile sample for analysis.
41.
PTC todecompress, assess proximal dilated
obstructed biliary system if ERCP fails; dine
polythene catheter can be kept in situ to
have biliary drainage;
PTC-stenting across the obstruction can be
done under image (C-arm) guidance.
MRCP-Noninvasive diagnostic tool. It shows
96% sensitivity; 99% specificity.
CT scan in case of tumours to assess
operability.
42.
Tumour markers:CA 19/9 is useful for
carcinoma pancreas (more than 70
units/L).
Endoscopic US (EUS): It is done through
endoscope.
It is more accurate in assessing
pancreatic mass, staging of the disease,
to identify involvement of portal venous
system, CBD stones.
43.
It isalso useful in EUS-guided FNAC,
celiac axis neurolysis, EUS-guided
immunotherapy.
lntraductal US (/DUS): It is very useful
in assessing tumour stage, tumour
margin in bile duct cancer.
It is also used in assessing pancreatic
duct to differentiate pancreatic cancer
and chronic pancreatitis.
44.
CT/MR angiogramor venogram to assess
vascularity and portal venous system in
malignancy.
Urine tests: Fouchet's test for bile
pigments, Hay's test for bile salts and test
for urobilinogen in urine.
Fouchet's test: 1 0 ml of urine+ 5 ml of
BaCl2+ pinch of MgSO4 causes formation of
BaSO4 which is filtered over a filter paper
and few drops of Fouchet's reagent is added.
45.
Green or bluecolour signifies presence of
bile pigments in the urine.
Hay's test for bile salt: Sprinkle sulphur to 2
ml of urine. In presence of bile salts sulphur
sinks to the bottom.
Ehrlich's test: 5 ml of freshly voided urine +
1 ml of Ehrlich reagent (p-dimethyl amino
benzaldehyde) and wait for 5 minutes.
Formation of red colour signifies presence
of urobilinogen in urine.
46.
Normally itis present in traces; in
obstructive jaundice, it is absent; and in
haemolytic jaundice, it is in excess.
48.
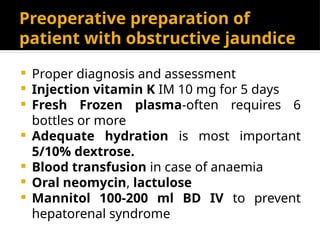
Preoperative preparation of
patientwith obstructive jaundice
Proper diagnosis and assessment
Injection vitamin K IM 10 mg for 5 days
Fresh Frozen plasma-often requires 6
bottles or more
Adequate hydration is most important
5/10% dextrose.
Blood transfusion in case of anaemia
Oral neomycin, lactulose
Mannitol 100-200 ml BD IV to prevent
hepatorenal syndrome
49.
Repeated monitoringby doing
prothrombin time, electrolytes.
Antibiotics like third generation
cephalosporins.
Calcium supplements as calcium
chloride IV.
Preoperative decompression is
indicated if bilirubin is> 12 mg%, sepsis,
hepatorenal syndrome, severe
malnutrition or cardiopulmonary
50.
Correction ofcoagulopathy,
prevention of renal failure, infection,
hepatic encephalopathy and
electrolyte imbalance (correction of
hypoglycaemia and dilutional
hyponatraemia due to water retention;
avoiding isotonic saline infusion).
51.
Treatment of Obstructive
Jaundice
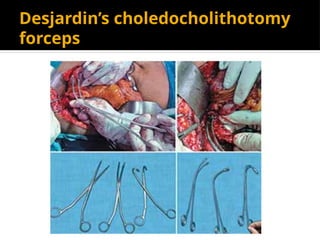
CBD stones-ERCP stone removal,
choledocholithotomy, transduodenal
sphincteroplasty, choledochojejunostomy
or choledochoduodenostomy.
Carcinoma periampullary or head of
pancreas-Whipple's operation or triple
bypass or ERCP stenting.
Biliary stricture-stenting,
choledochojejunostomy, Rouxen-Y
hepaticojejunostomy.
It includesa group of malignant tumors
arising at or near the ampulla: „
Adenocarcinoma from head of
pancreas adjacent to the ampulla
(within 2 cm.
Ampullary tumor.
„Distal bile duct carcinoma „
Duodenal carcinoma adjacent to the
ampulla.
56.
Etiological factors fordevelopment
of carcinoma pancreas
Smoking
Alcohol
Diet: Diet high in protein and fats.
Chronic pancreatitis
Diabetes
Genetic: BRCA2 gene.
57.
Clinical features
Painlessprogressive jaundice
Epigastric pain: Dull aching epigastric
pain, radiating to the back,worse at
night and in supine position with some
relief in leaning forwrad.
Nonspecific symptoms: Malaise, weight
loss, nausea and vomiting. „
Diarrhea or steatorrhea. „
New onset diabetes mellitus.
58.
Normal dimension ofpancreatic
duct
In the head region—5 mm
In the body—3 mm
In the tail—2 mm.
59.
Rarely patientmay present with S/S of
„
acute pancreatitis.
Migratory thrombophlebitis (Trousseau
sign).
60.
Resectable tumor
Tumorlocalized to the pancreas „
No evidence of SMV or portal vein
involvement „
Preserved fat plane between the tumor
and the SMA and celiac trunk branches
„
No evidence of distant metastasis.
61.
Borderline resectable
disease
Unilateralor bilateral SMV-PV
impingment. „
Less than 180 degree tumor abutment
on SMA. „
Abutment or encasement of hepatic
artery, if reconstructible. „
Short segment occlusion of SMV, if
reconstructible.
62.
Signs of inoperability
Ascites „
Peritoneal metastasis „
Multiple liver metastasis „
Extensive lymph node metastasis „
Invasion of growth to IVC Invasion of
„
growth to superior mesenteric vessels,
portal vein or celiac axis.
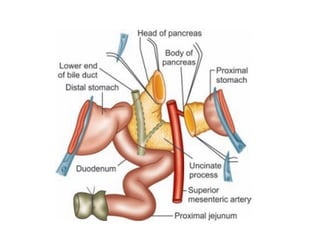
63.
Structures will removein
Whipple’s
Whole of duodenum up to 10 cm of
proximal jejunum „
Head and neck of pancreas including
uncinate process „
Distal 40–50% of stomach „
Lower end of common bile duct (CBD) „
Gallbladder „
Pericholedochal, periduodenal and
peripancreatic lymph nodes.
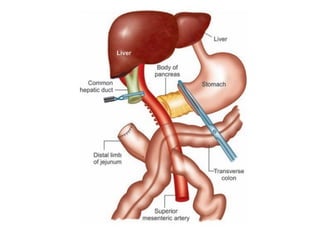
64.
Maintain continuity following
resectionfor Whipple’s operation
Pancreaticojejunostomy (end to side)
Hepaticodochojejunostomy (end-to-
side) 10–15 cm beyond the
pancreaticojejunostomy
Beyond 10–15 cm of
hepaticodochojejunostomy
gastrojejunostomy
65.
Steps of Whippleoperation
Anesthesia
Position of the patient
Antiseptic cleaning and draping
Incision
Exploration of abdomen
Assessment for resectability
Exposure of the duodenum and the
head of the pancreas
Kocherisation of duodenum
66.
Exposure of thepancreas
Exposure and dissection of superior
mesenteric vessels
Dissection of hepatoduodenal ligament
and portal structures
Cholecystectomy and division of bile
duct
Division of gastrohepatic omentum and
lymph nodes
Distal gastrectomy
67.
Division ofthe neck of the pancreas
Division of the jejunum
Division of uncinate process
Removal of specimen
Reconstruction
Pancreaticojejunal anastomosis
Hepaticodochojejunostomy
Gastrojejunal anastomosis
Closure of transverse mesocolon rent
Primary bile ductstones
Stones that form in bile duct itself.
The bacterial enzyme hydrolyzes
bilirubin diglucuronide into free
bilirubin which then precipitates and
form a complex with cholesterol.
Principal composition of the pigment
stone is calcium bilirubinate.
Pigment stones are either brown or
black.
79.
Brown stonesare associated with
infection in the biliary tree.
Black stones are associated with
chronic hemolytic diseases.
80.
Secondary bile ductstones
Stones that form in gallbladder and
then migrate into the bile duct.
81.
Retained or residualbile duct
stones
Stones in the bile duct detected within
two years following cholecystectomy.
Stones missed during cholecystectomy
with or without bile duct exploration.
Stones have the characteristics of
secondary bile duct stones.
82.
Recurrent bile ductstones
Stones which form within the bile duct
2 years after initial operation.
It has the characteristics of primary bile
duct stones.
83.
Clinical features
Charcot'striad
„
Obstructive jaundice: Itching, clay
„
colored stool „
Associated pancreatitis may cause pain
in the back „
Abdominal tenderness may be present
in right upper quadrant during an
attack of cholangitis „
84.
Charcot’s triad
Intermittentpain
„
Intermittent jaundice. „
Intermittent fever.
It is triad of symptoms suggest
cholangitis.
85.
Reynold’s pentad
Charcoat’striad (Intermittent pain,
„
intermittent jaundice, intermittent
fever). „
Along with mental status changes and
evidence of shock (hypotension). !
It is is found in severe cholangitis with
septicemia.
90.
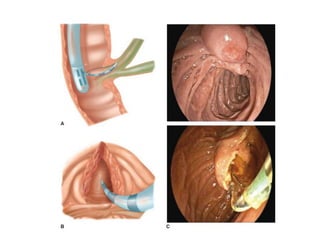
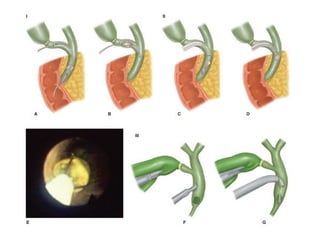
Treatment
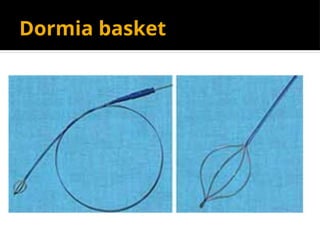
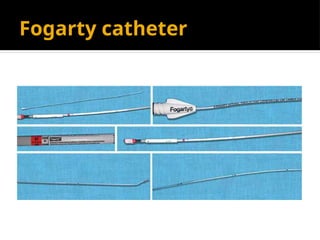
Endoscopic sphincterotomyand bile
duct stone extraction by a Dormia
basket catheter introduced through the
endoscope followed by laparoscopic
cholecystectomy.
In absence of such facilities
conventional open cholecystectomy
with bile duct exploration is the
standard operation.
93.
Problems with ERCPstone
extraction
Procedure may not be possible
„ „
Stones larger than 1. 5 cm is not
suitable for extraction endoscopically
unless there is facility for contact
lithotripsy. „
Risk of post procedure cholangitis,
pancreatitis, bleeding or rarely
duodenal perforation remains.
94.
Mechanical flushing
Ifthe retained stone is small (< 1cm).
Bile duct is irrigated with a heparinized
saline (250 mL of normal saline mixed
with 25,000 IU of heparin) by passing
the fluid through the T-tube tract for
consecutive 5 days.
An injection of hyoscine may relax the
ampulla of vater and may facilitate the
expulsion of small stones.
95.
Contact dissolution
Ifthe stone is a pure cholesterol one,
contact dissolution by infusing
monooctanoin or methyl terbutyl ether
via the T-tube tract.
96.
Burhene technique
Patientis discharged home with the T-
„
tube in situ, and a waiting period of 4–6
weeks allows the T-tube tract to get
matured. „ „
A Dormia basket catheter is introduced
through the T-tube tract into the bile
duct and the stones may be removed. „
Risk factors
Gallstonedisease.
Choledochal cyst.
Anomalous pancreaticobiliary duct
junction.
Gall bladder polyp >1 cm.
Adenomyomatosis of gallbladder.
Chronic typhoid carriers
Carcinogenes, e.g. nitrosamines.
107.
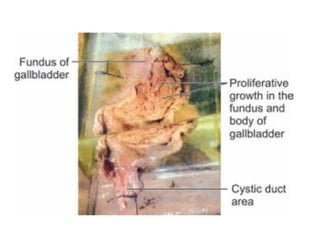
Clinical features
Symptomsand signs suggestive of acute
cholecystitis.
Symptoms and signs of chronic biliary tract
disease—right upper quadrant pain,
jaundice.
General symptoms and signs suggestive of a
malignant disease—anorexia, weight loss,
generalized weakness.
Symptoms and signs suggestive of disease
outside the biliary tract—gastric outlet obstr-
108.
uction and gastrointestinalbleeding.
Symptoms and signs suggestive of
advanced malignant disease—palpable
gallbladder mass, hard nodular liver and
ascites. „
Carcinoma of gallbladder is suspected in a
patient who has long standing history of
gallstone disease in which a recent change
in symptomatology and pain has occurred.
109.
TNM staging
Primary tumor(T)„
Tx- Primary tumor cannot be assessed. „
T0- No evidence of primary tumor. „
Tis- Carcinoma in situ. „
T1- Tumor invades lamina propria or
muscular layer.
T1a- Tumor invades lamina propria.
T1b- Tumor invades muscularis propria.
„
110.
T2-Tumor invadesperimuscular
connective tissue. No extension beyond
serosa or into the liver.
T3-Tumor invades beyond the serosa.
Tumor invades into the liver.
Tumor invades into one adjacent organ
—stomach, duodenum, colon, pancreas,
omentum or extrahepatic bile duct.
111.
T4-Tumor invadesportal vein or hepatic
artery and two or more extrahepatic organ
or structure.
Regional lymph nodes (N): „
Nx:- Regional lymph nodes cannot be
assessed. „
N0- No regional lymph node metastasis. „
N1- Metastasis to nodes along the cystic
duct, common bile duct, hepatic artery or
112.
or portal vein.
N2- Metastasis to periaortic, pericaval,
superior mesenteric arteryand or/celiac
artery lymph nodes.
Distant metastasi (M): „
M0- No distant metastasis. „
M1-distant metastasis present.
113.
Structures to removein radical
cholecystectomy
Cholecystectomy with a 2 cm wedge of liver
tissue at the gallbladder bed to ensure a
tumor free margin.
Some advocates resection of segments V and
IVb. „
Lymph node dissection removing
pericholedochal, periportal, hepatoduodenal,
nodes along the hepatic artery, portal vein,
lymph nodes behind 2nd part of duodenum,
peripancreatic nodes around the head of
Non resectable
Patientfactors:
1. Age: Elderly patient tolerate radical
surgery poorly
2. Poor general condition
3. Comorbid condition
4. Sepsis.
Tumor factors:
Distant metastasis: Intraperitoneal or
extraabdominal
117.
2. Extensive metastasisin both lobes of
the liver
3. Invasion of growth into the portal
vascular structures
4. Invasion of growth into the
duodenum, pancreas or colon.
Etiological factors
Stonedisease: bile duct stones.
„ „
Bacterial induced endogenous
carcinogenes in the bile.
Sclerosing cholangitis and ulcerative
colitis.
Choledochal cyst
„
Parasitic infestation of bile duct :
Clonorchis sinensis.
121.
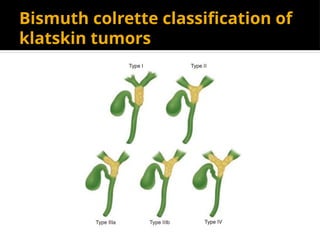
Types of
cholangiocarcinoma
Depending onthe sites of involvement of the
biliary tree :
Intrahepatic.
Extrahepatic
−Proximal: Arises either from right or left
hepatic ducts or the confluence or the proximal
common hepatic duct (Klatskin’s tumor)
−Middle: Involves the common hepatic duct
and the proximal common bile duct
−Distal: From distal common bile duct and the
periampullary region.
122.
−Distal: From distalcommon bile duct
and the periampullary region.
Depending on the gross appearance
Scirrhous type: causes diffuse thickening
of wall of the bile duct.
Nodular variety.
Papillary variety: Mainly involves the distal
bile duct and the periampullary region.
123.
Friable vascular growthmay fillll the
bile duct lumen and bleeds easily
leading to hemobilia.
Histological types „
Majority are adenocarcinoma. „
Rare types may include squamous cell
carcinoma, adenosquamous cell
carcinoma, lymphoma, carcinoid,
melanoma and very rarely APUDOMAS.
Clinical features
Obstructivejaundice.
„
Dull upper abdominal pain „
Anorexia, weight loss „
May present with acute cholangitis „
Gallbladder may be palpable in distal
bile duct lesion.
126.
Treatment
Advanced disease:Palliative treatment
for relief of jaundice either by surgical
bilioenteric bypass or endoscopic
stenting or percutaneous transhepatic
biliary drainage (PTBD).
Inoperable hilar lesion: Surgical
bilioenteric bypass (Anastomosis of a
Roux-en-Y loop of jejunum to segment
III duct)
127.
Middle cholangiocarcinoma:excision
extending from below the confluence of the
hepatic duct down upto the duodenum along
with pericholedochal lymph nodes.
Distal or periampullary cholangiocarcinoma:
Whipple pancreaticoduodenectomy.
Klatskin’s tumor: Excision of the tumor with
both right and left hepatic duct anastomosis
with a Roux en Y loop of jejunum.
Theories
First theory:Babbit hypothesis. There is
anomalous pancreaticobiliary duct junction.
there is reflux of pancreatic juice into the
bile duct. It causes increase in pressure in
the bile duct and also there is enzymatic
destruction of bile duct wall leading to
ductal weakening and dilatation.
Second theory: Abnormal canalization of
bile duct during embryogenesis with distal
obstruction. The distal obstruction causes
131.
increased proximal pressureleading to
ductal dilatation. „
Third theory: Pathogenesis of
choledochal cyst involves abnormalities
of autonomic innervation of the
extrahepatic biliary tree. There is
reduction of postganglionic neurons in
the narrow distal portion of the cyst in
comparison to the dilated part of the
cyst.
132.
Clinical features
Classictriad of choledochal cyst: „
Jaundice „
Right upper quadrant mass and „
Right upper quadrant abdominal pain.
Other symptoms are: Nausea, pruritis and
weight loss. „
Adults may present with: features of acute
pancreatitis or acute cholangitis. „
May rarely present with acute rupture of the
cyst with S/S of acute biliary peritonitis.
133.
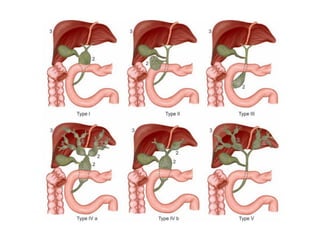
Todani classification
TypeI:Dilatation of extrahepatic biliary
„
tree—Ia-Cystic, Ib-Focal, Ic-Fusiform. „
Type II: Saccular diverticulum of
extrahepatic bile duct. „
Type III: Dilatation of intraduodenal
part of bile duct—Choledochocoele. „
Type IVa: Dilatation of both intrahepatic
and extrahepatic biliary tree.
Type IVb: Multiple extrahepatic cysts.
„
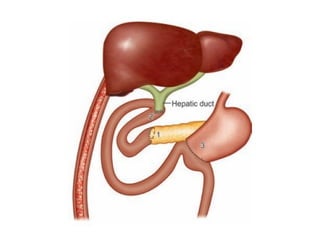
Treatment
Total excisionof the choledochal cyst and
hepaticodochojejunostomy with a Roux-en-Y
limb of jejunum.
Type III choledochal cyst (Choledochocele) is
treated either by transduodenal
sphincteroplasty or sphincterotomy.
Type V(Caroli’sdisease) „
Confined to one lobe or segment—lobectomy
or segmental resection „
Di#use disease involving both lobe —liver
transplantation.

![ Extrahepatic obstruction may be
Luminal (stones, infestations [ascariasis,
clonorchis sinensis and schistosomiasis) or
Mucosal/wall (growth, stricture [post-
inflammatory, postsurgical or post-RT],,
primary sclerosing cholangitis) or
External compression (pancreatitis,
pancreatic tumour, compression by
nodal mass).](https://image.slidesharecdn.com/surgicaljaundiceobstructivejaundice-250303193333-29d13fca/85/SURGICAL-JAUNDICE-Obstructive-Jaundice-pptx-24-320.jpg)