Downloaded 1,977 times
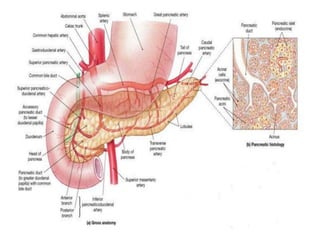
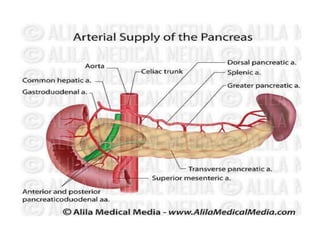
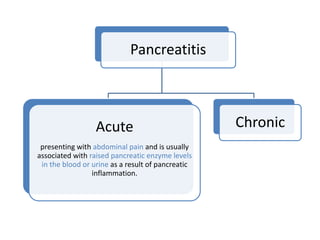
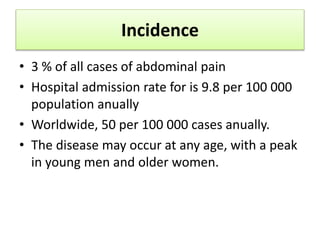



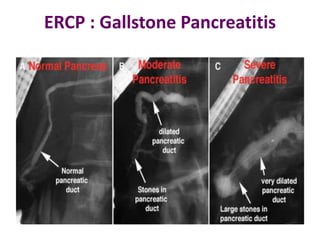
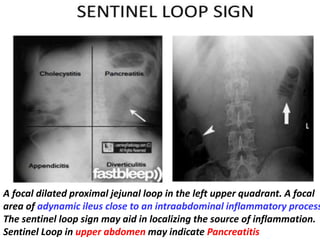
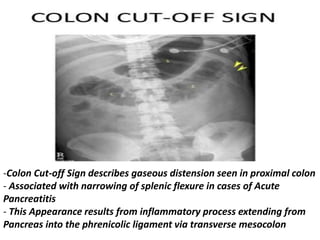

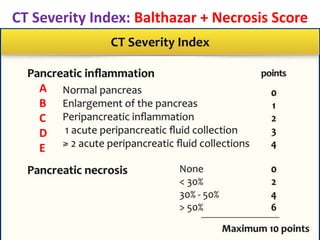
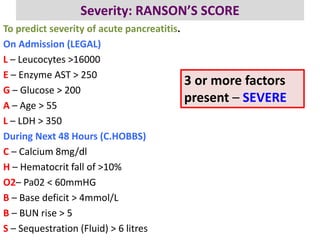
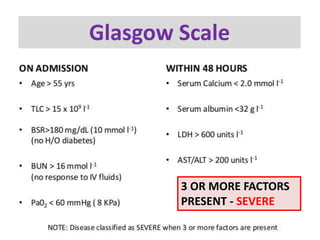
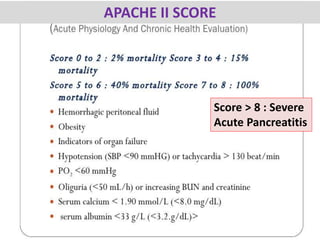

The document provides a comprehensive overview of acute pancreatitis, detailing its anatomy, aetiology, pathophysiology, clinical evaluation, differential diagnoses, and management strategies. It emphasizes the importance of history and physical examination in diagnosing the condition, common causes such as biliary calculi and alcohol abuse, and the various complications that may arise. The document also outlines the severity assessment using various scoring systems and discusses diagnostic imaging techniques involving ultrasound, CT scans, and ERCP.

































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)















