Downloaded 205 times
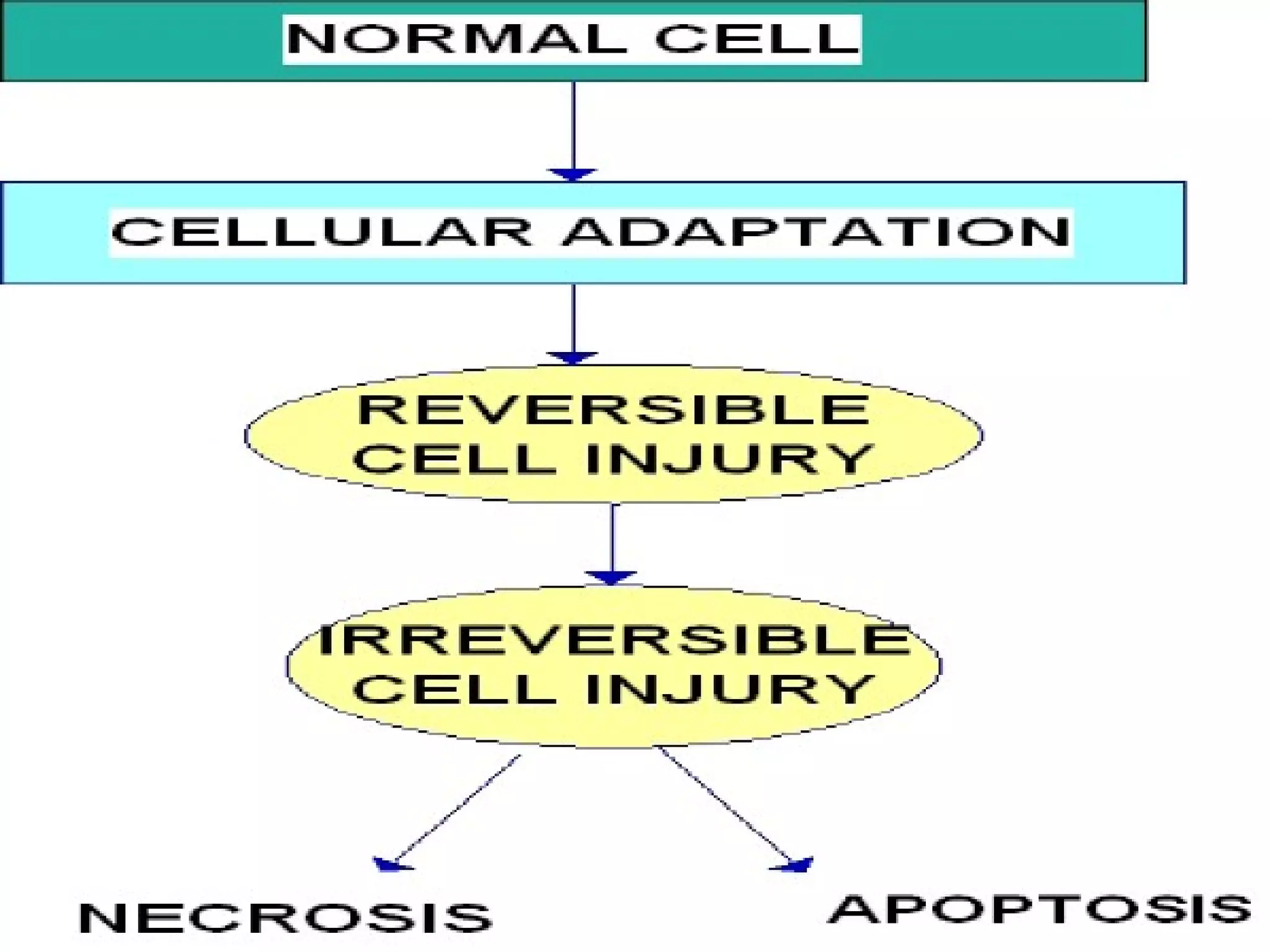
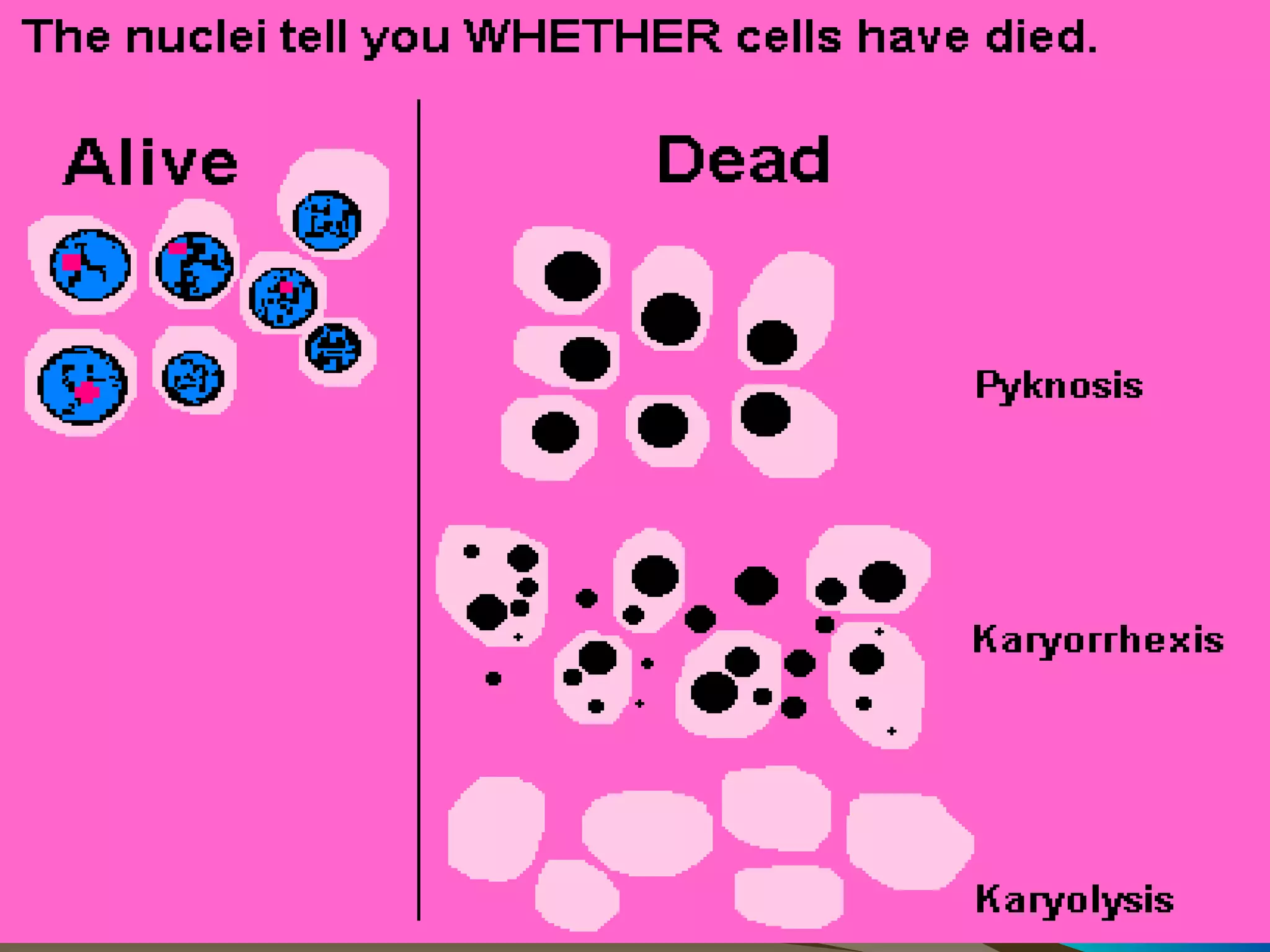
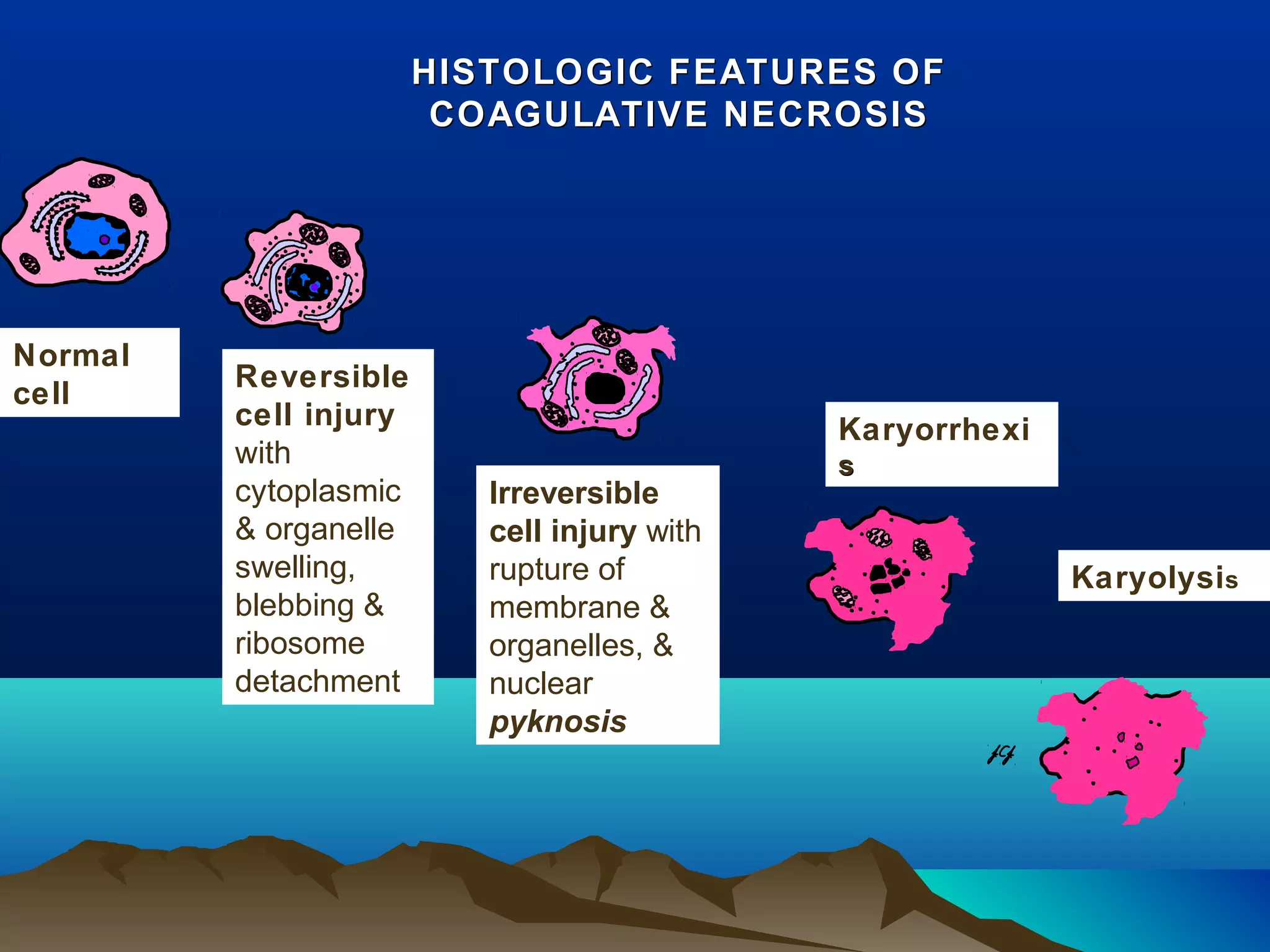
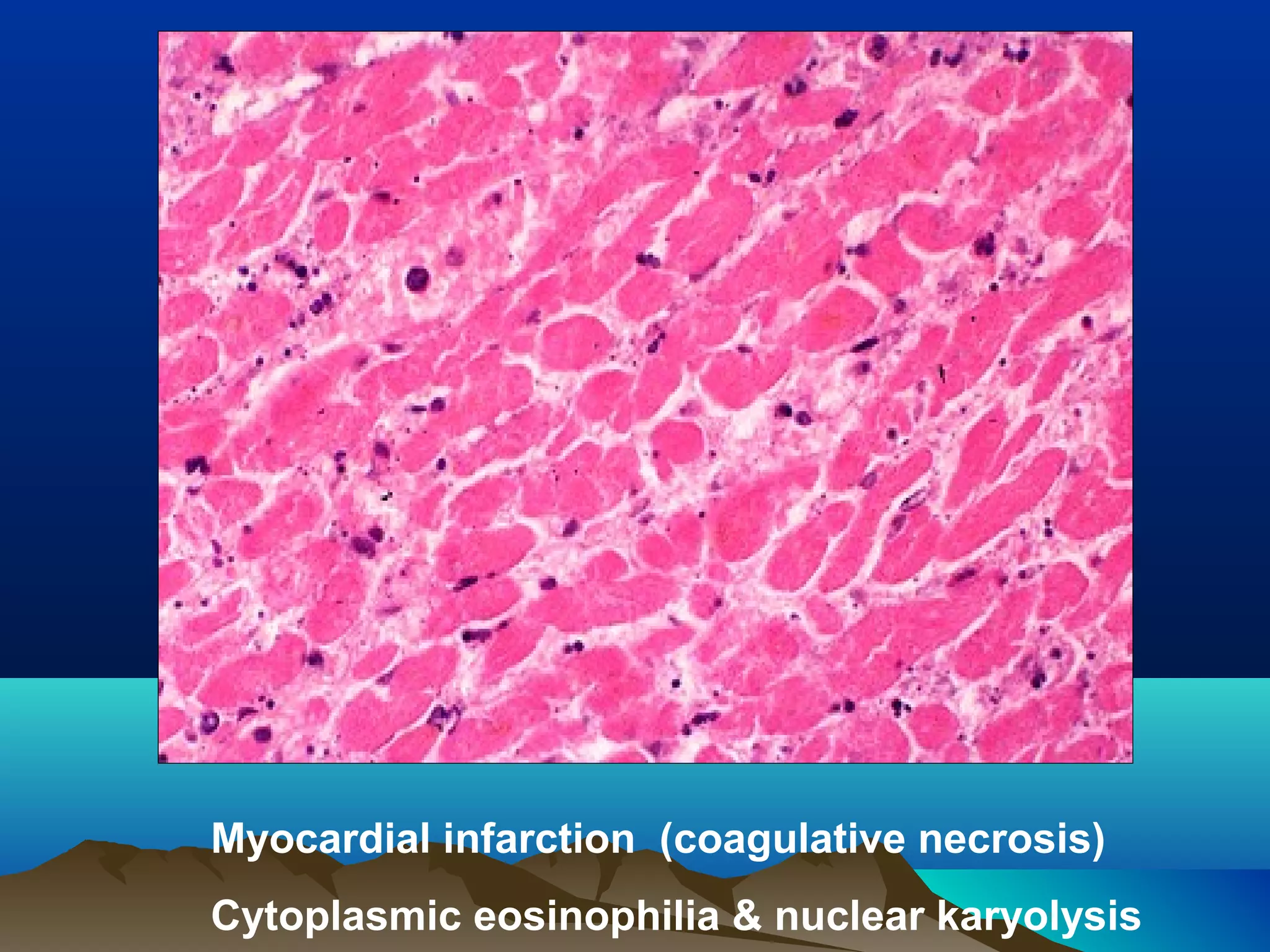

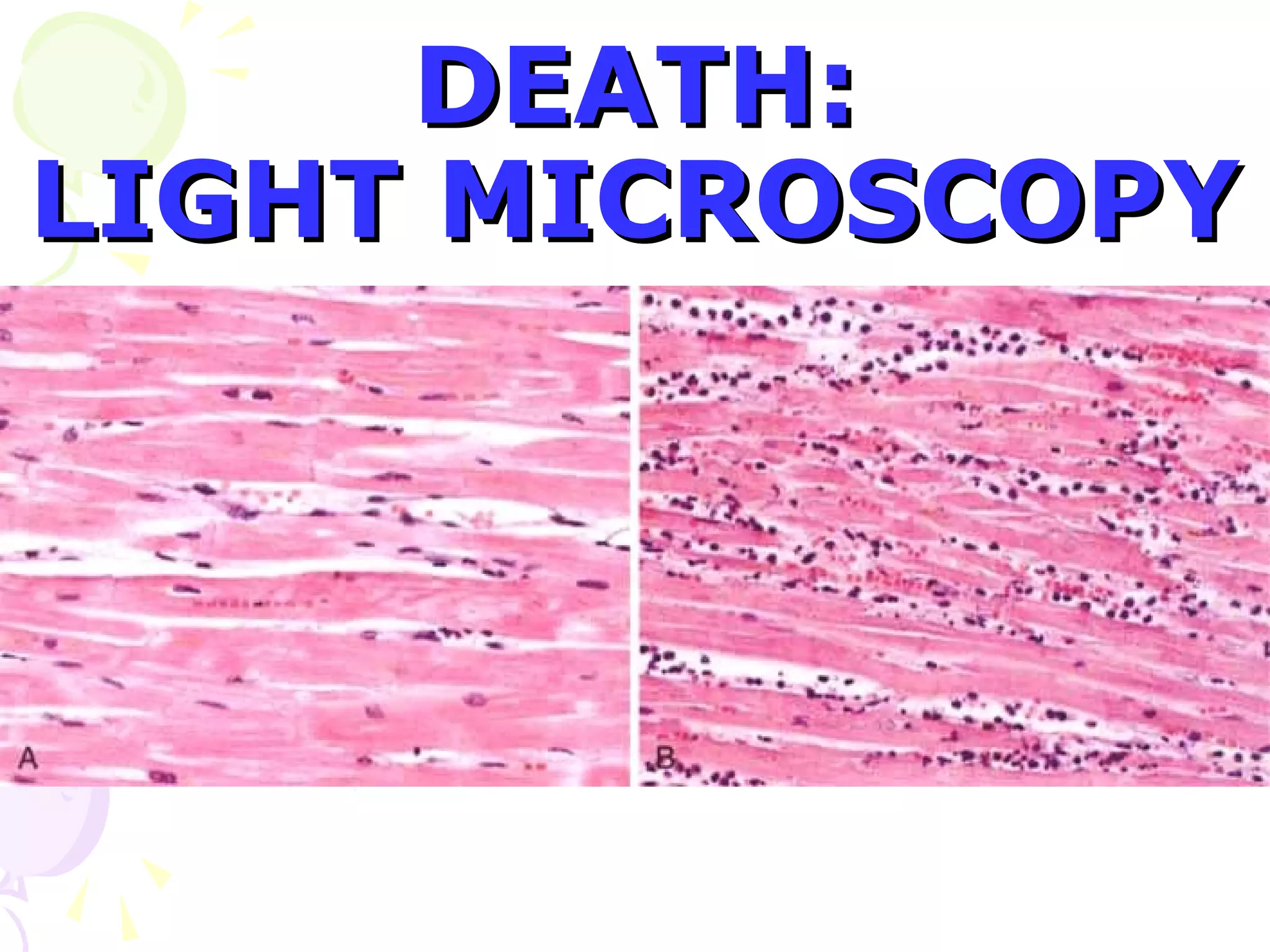
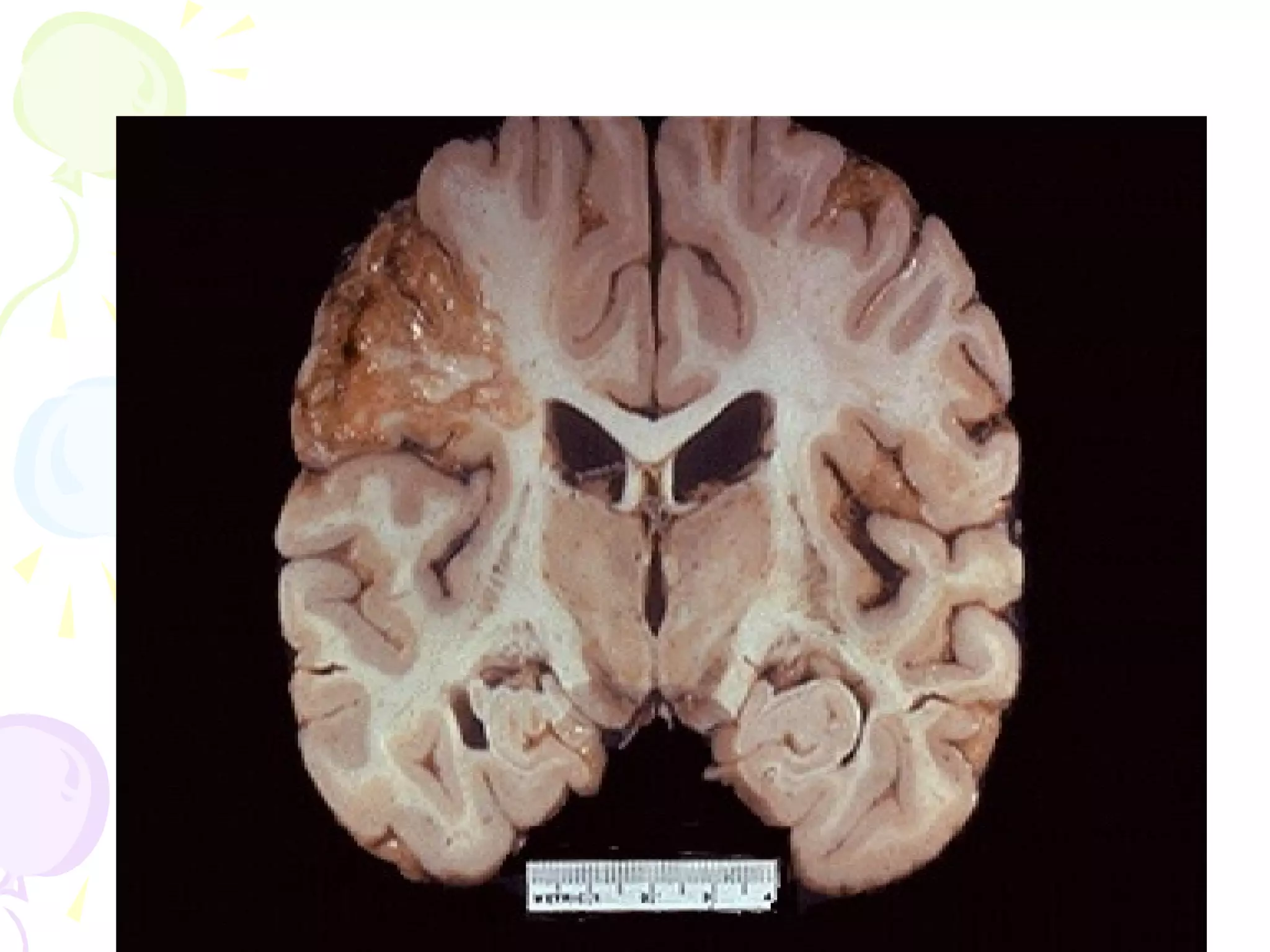
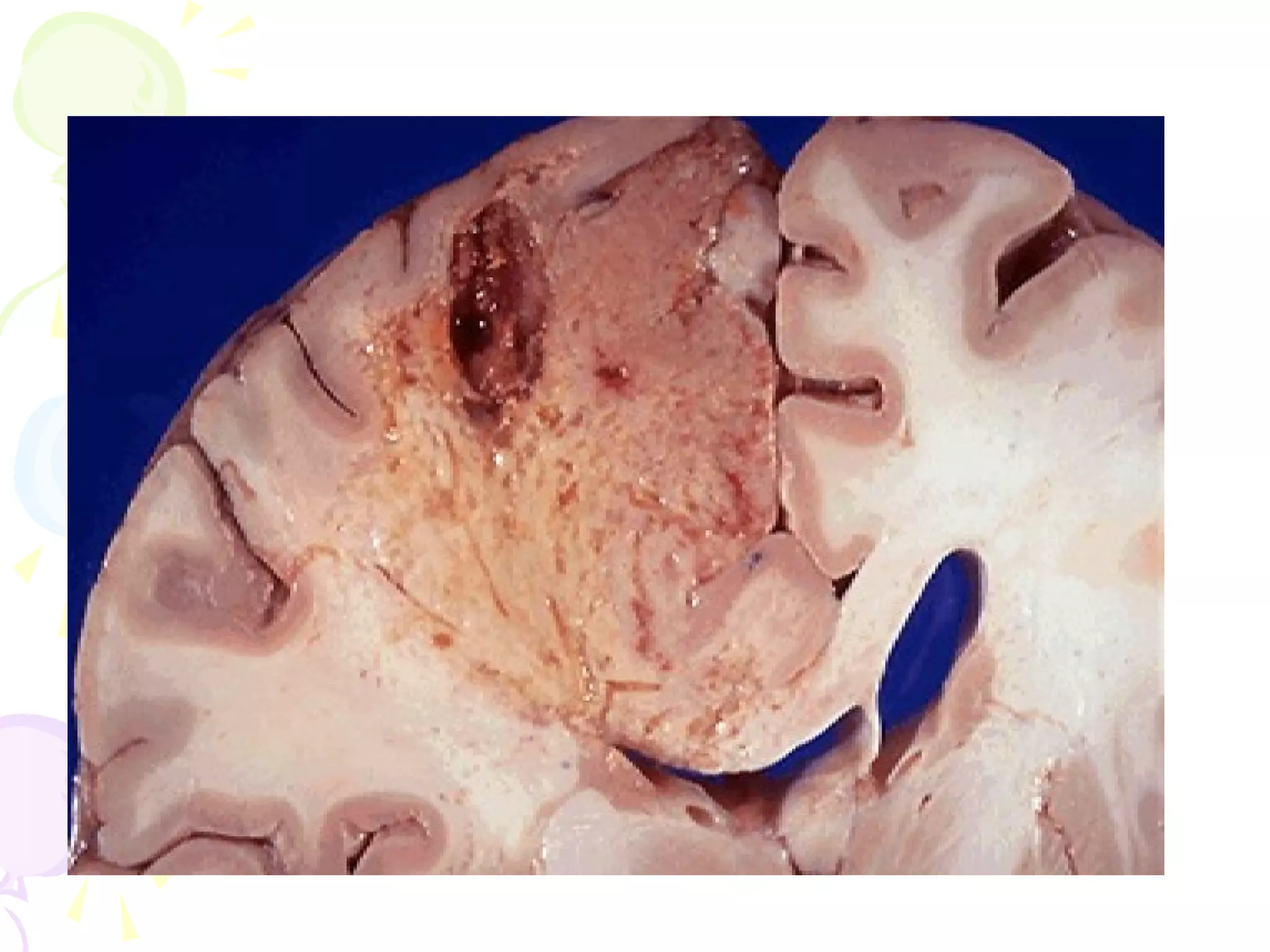
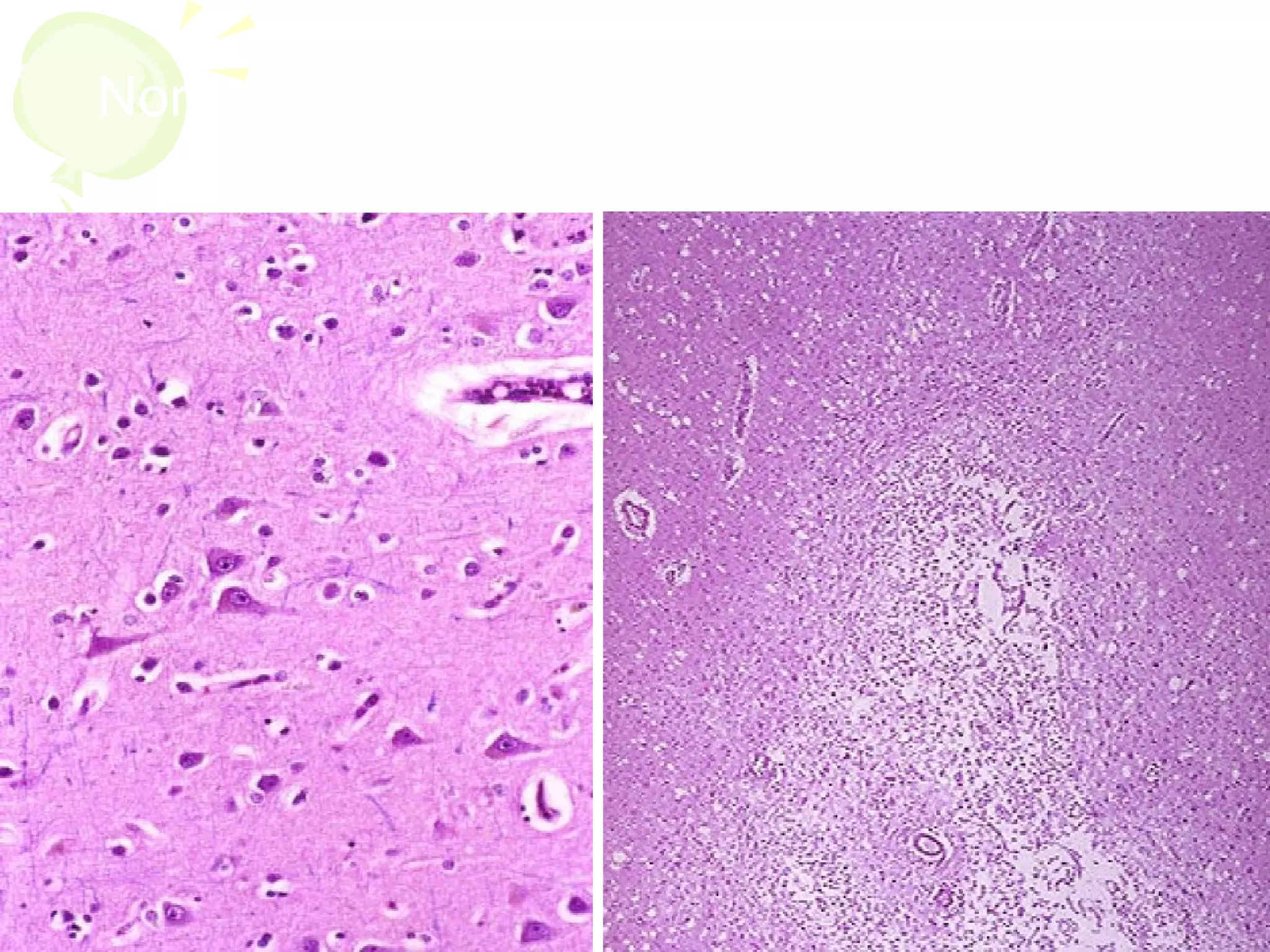
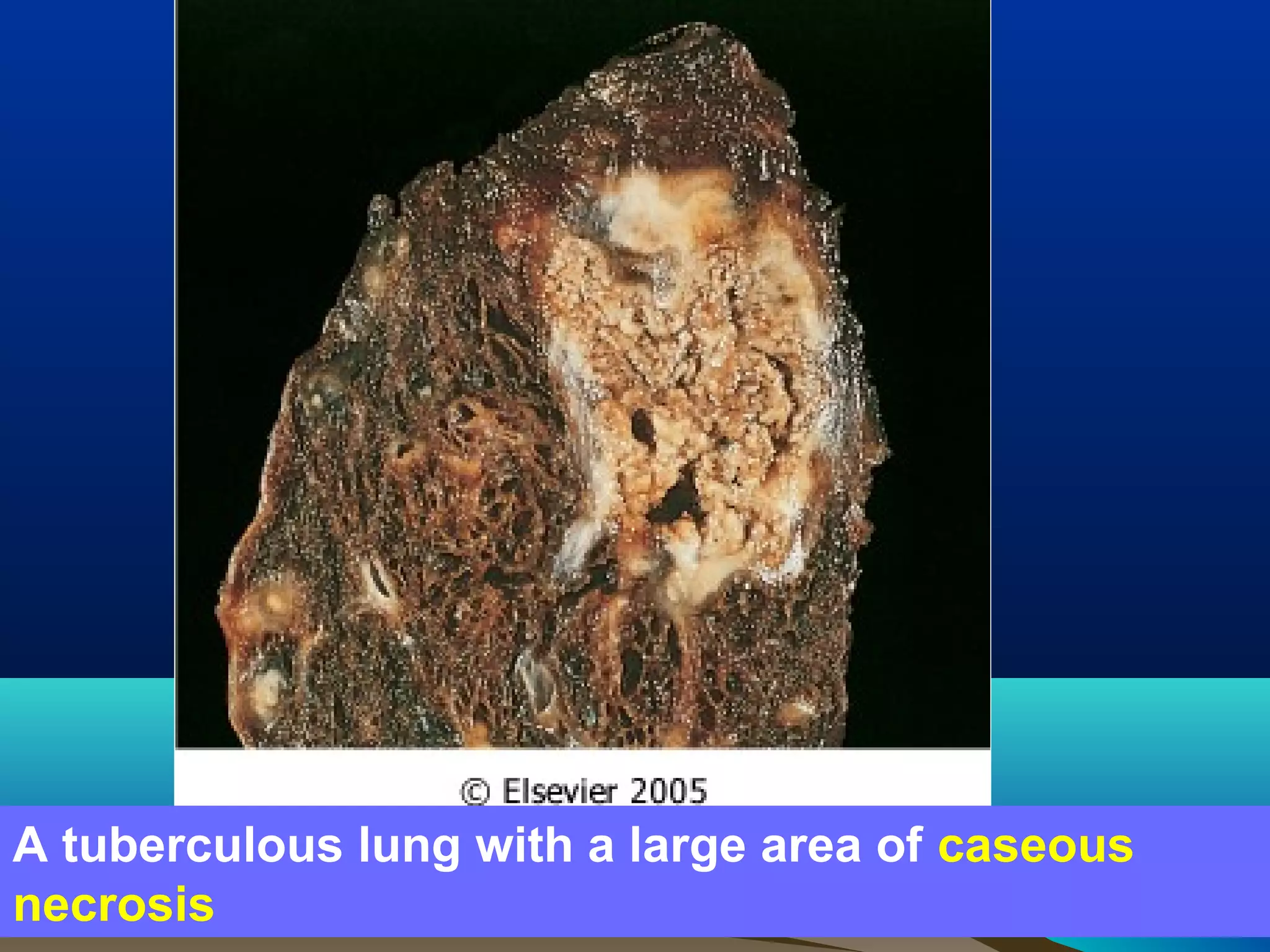
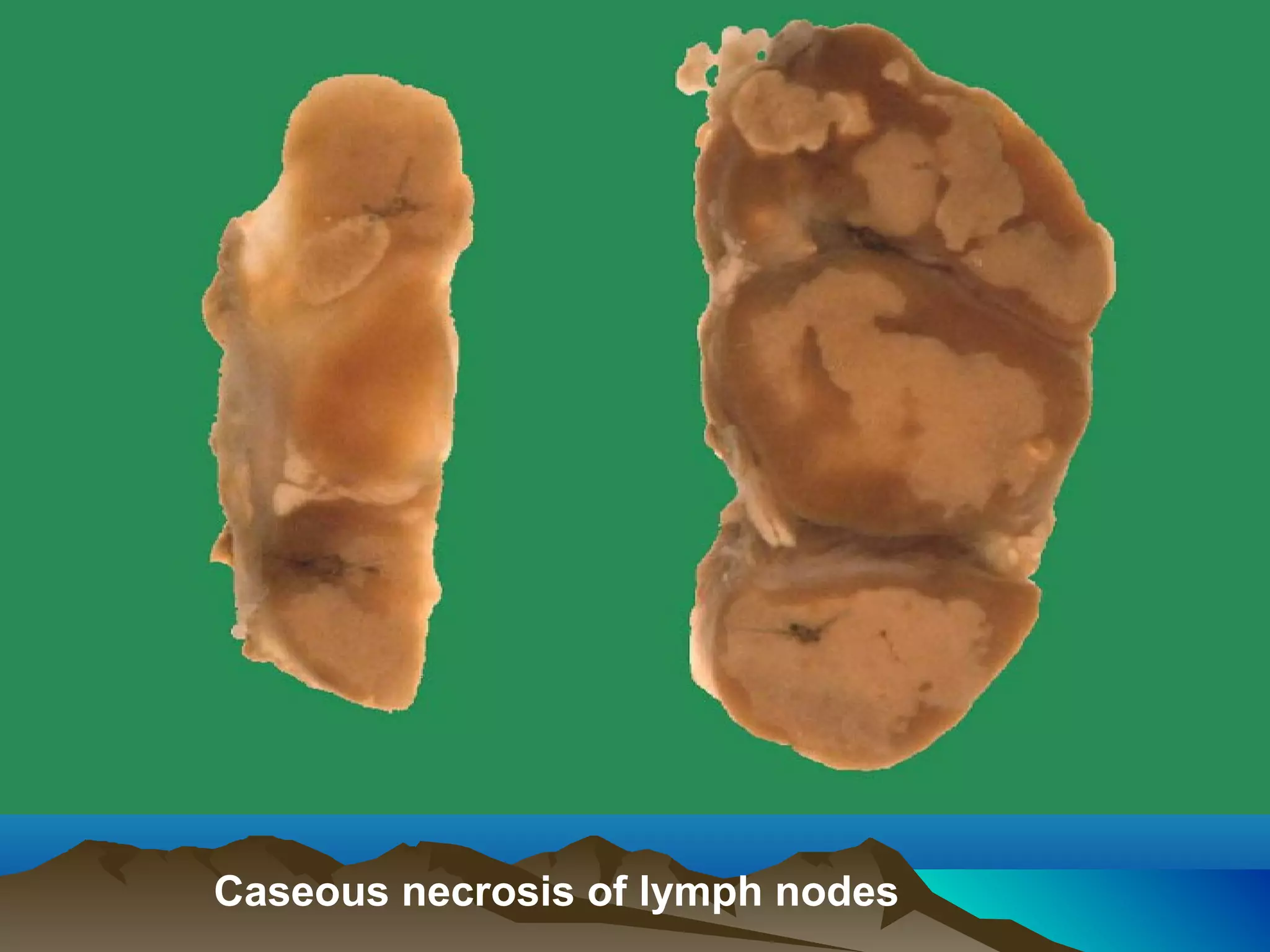
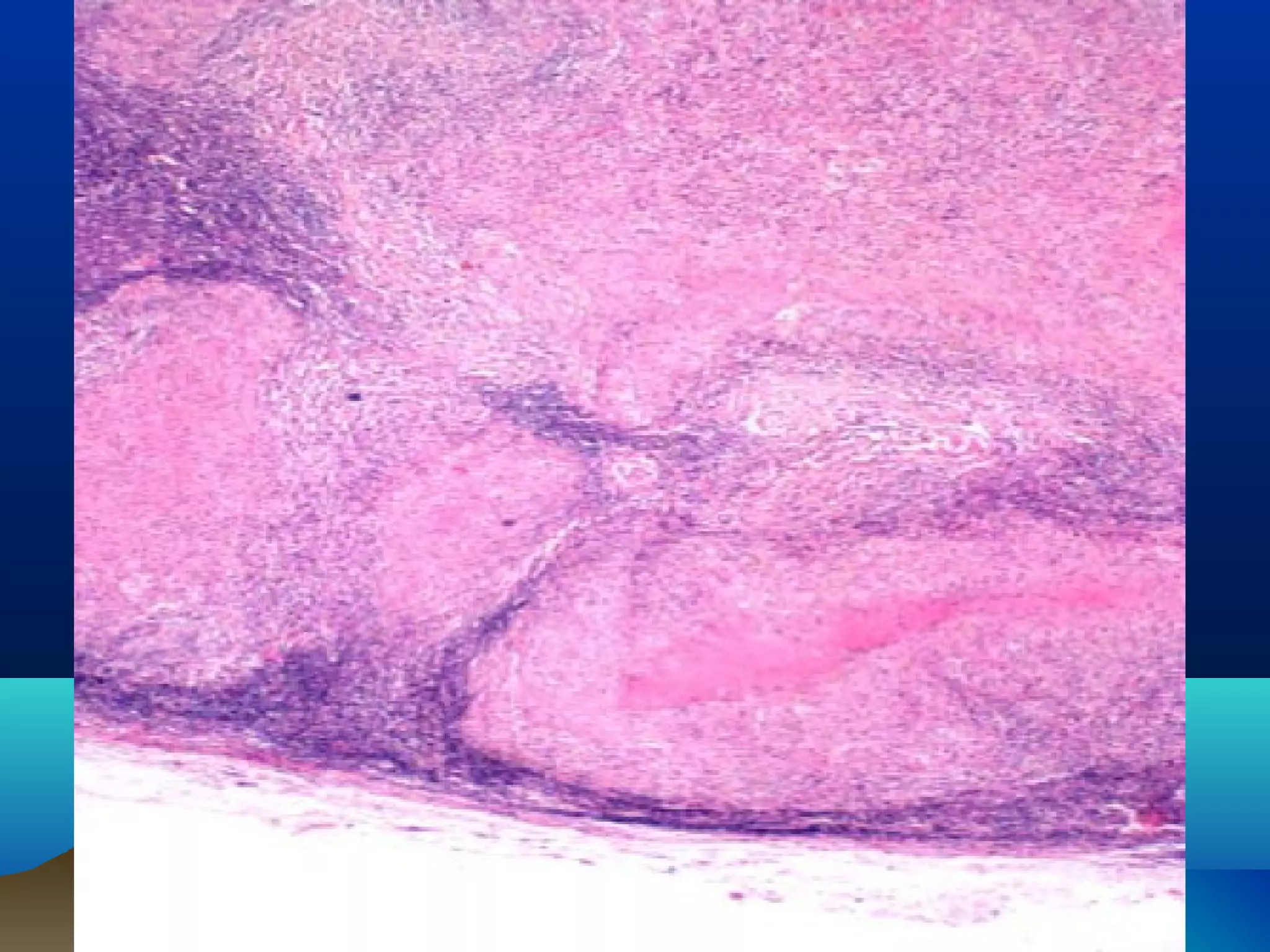
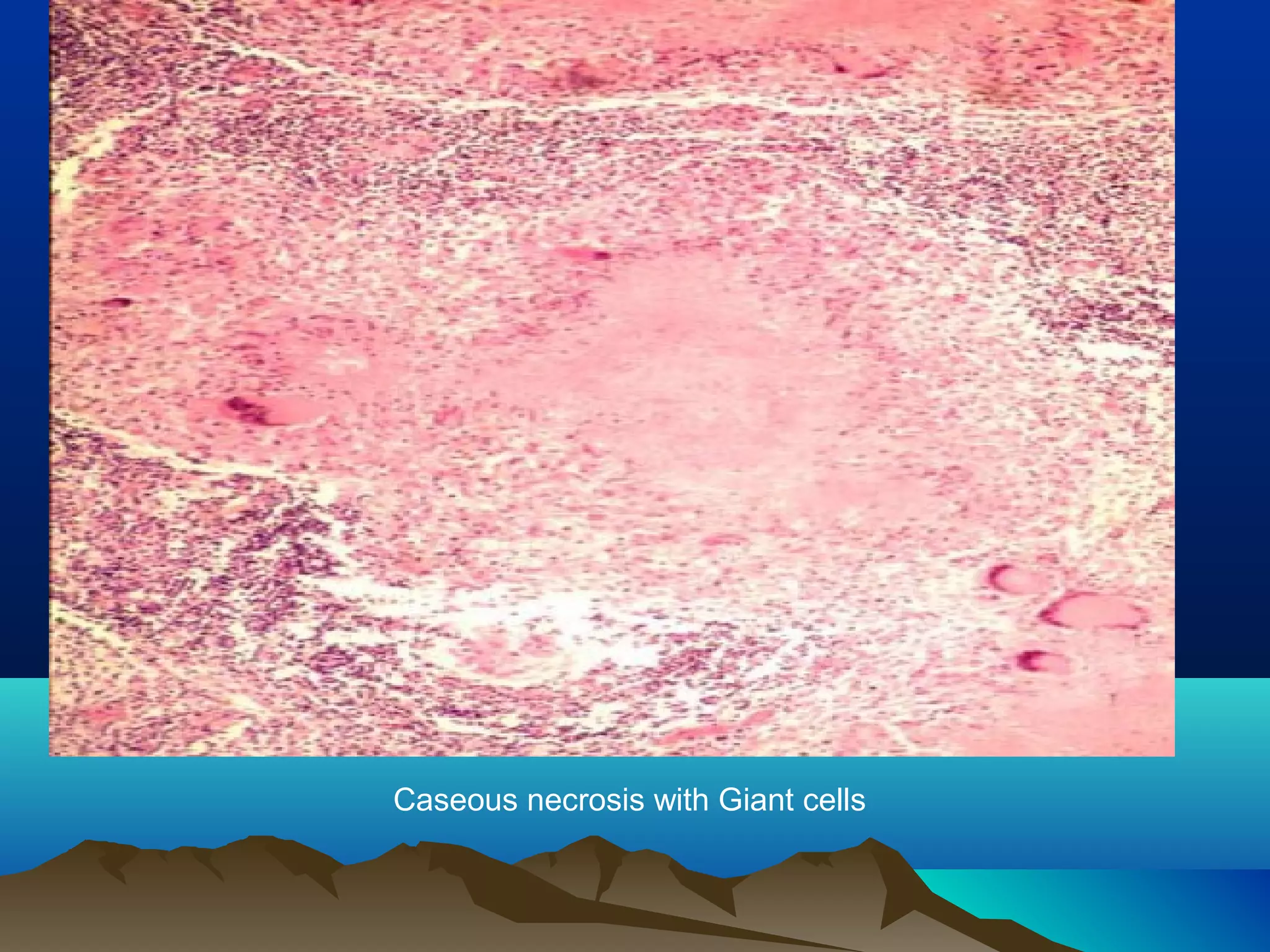
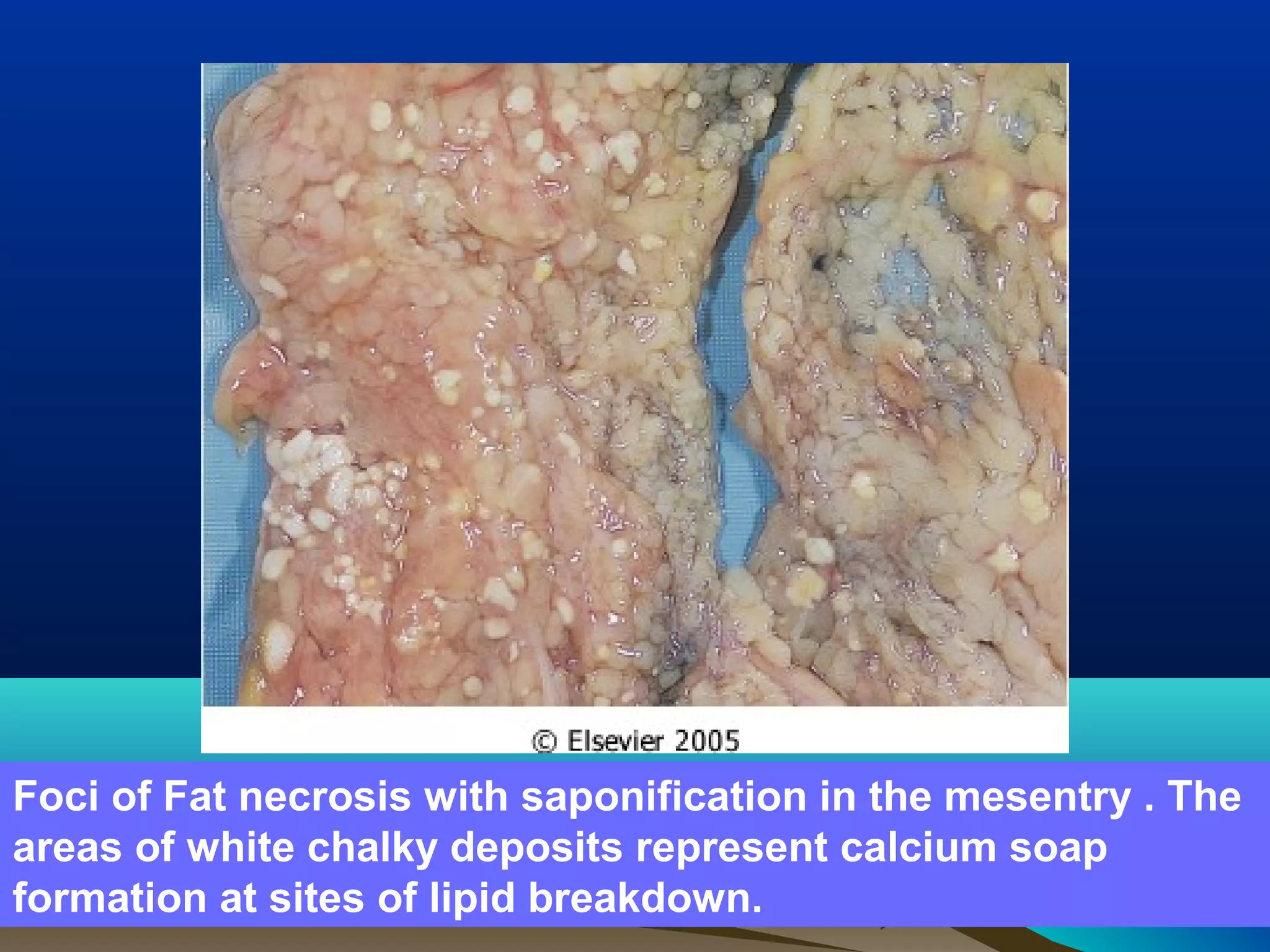
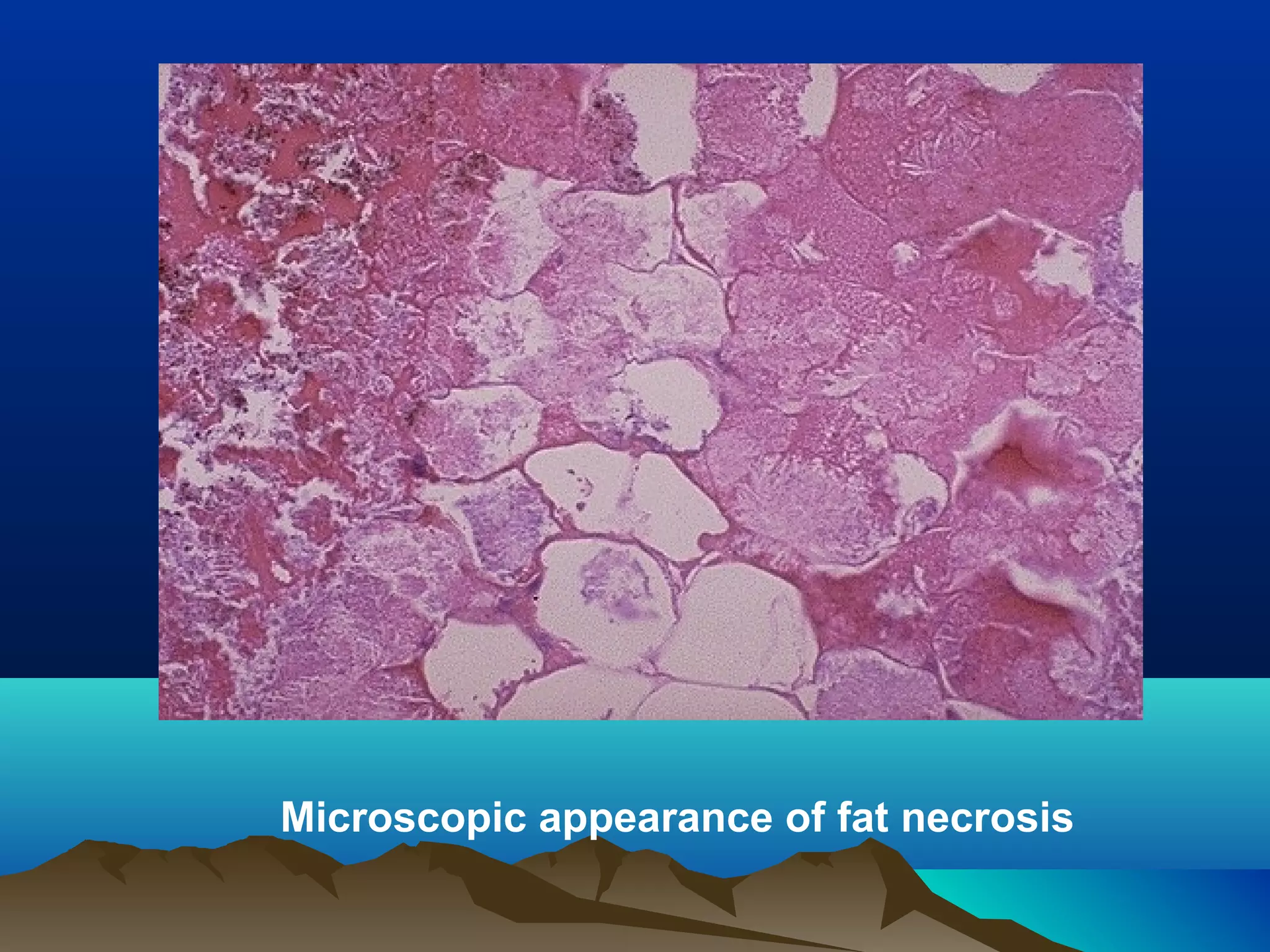



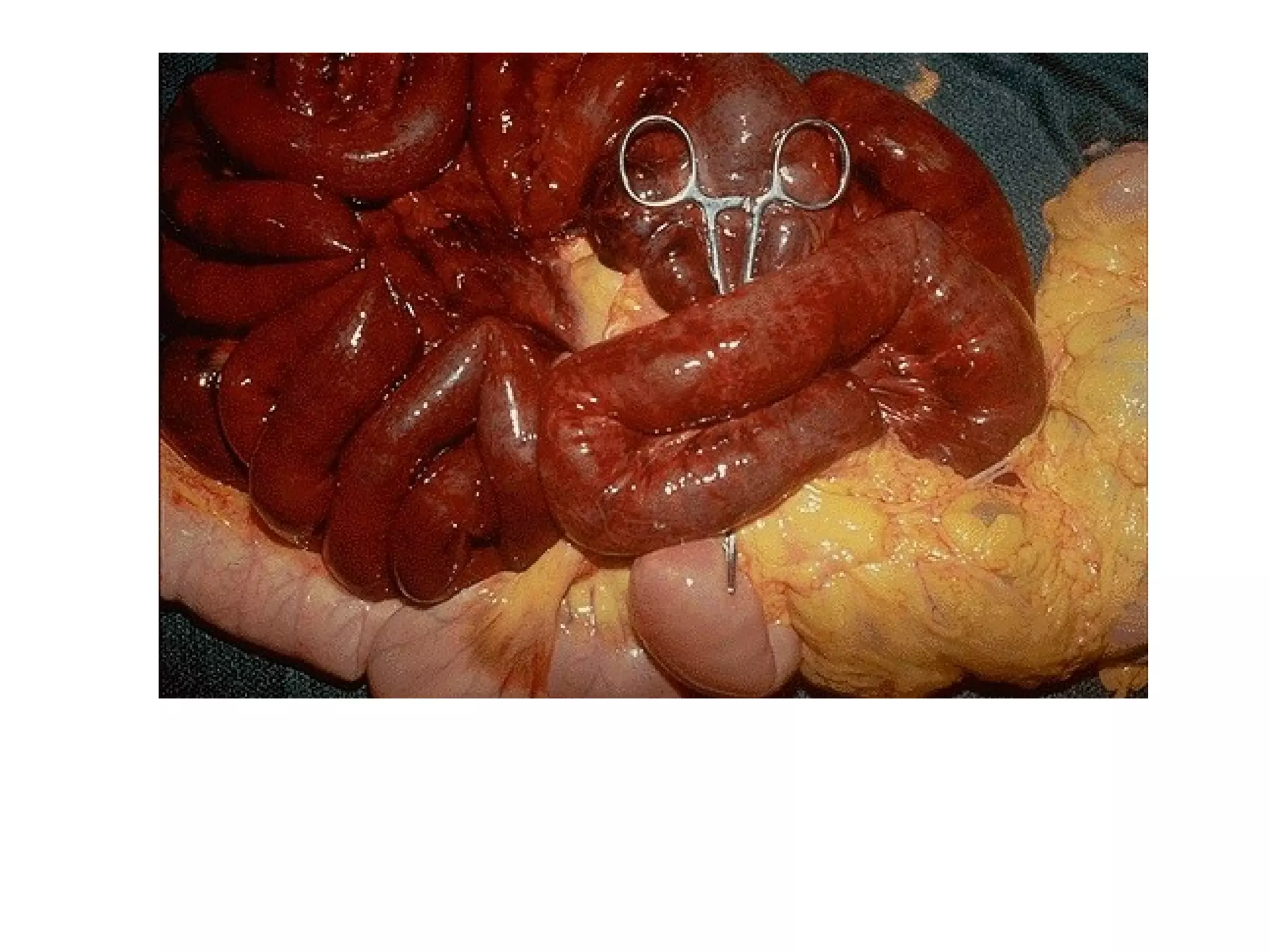

This document discusses different types of cell death, including apoptosis and necrosis. It describes necrosis as cell death resulting from external factors that cause irreversible injury. The key morphological changes seen with necrosis include increased cytoplasmic eosinophilia, nuclear pyknosis, karyorrhexis, and karyolysis. There are several patterns of necrosis depending on the mechanism and tissue involved, such as coagulative, liquefactive, caseous, and gangrene. Coagulative necrosis preserves tissue architecture while liquefactive necrosis destroys tissue structure. Gangrene refers to visible tissue necrosis, usually due to ischemia.




















































































![Prac excises 3[1].5](https://cdn.slidesharecdn.com/ss_thumbnails/pracexcises31-150331131154-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)

