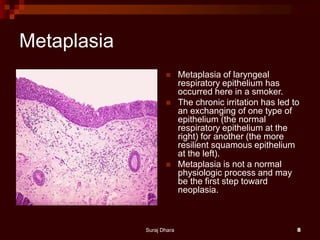
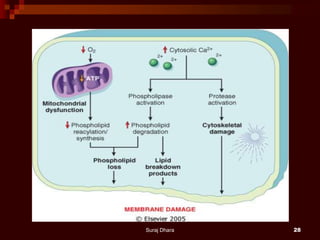
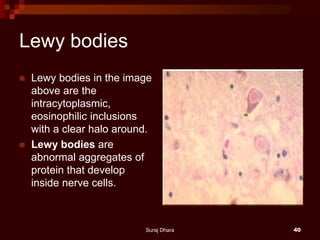
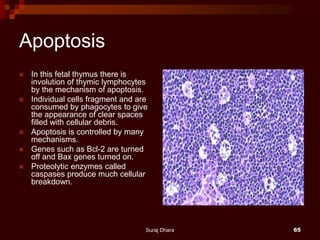
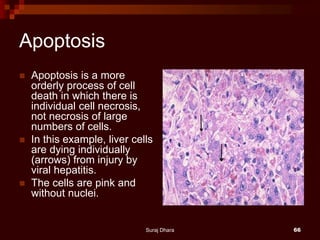
This document provides an overview of cellular adaptation and injury. It defines four types of cellular adaptation - atrophy, hypertrophy, hyperplasia, and metaplasia. It also lists common causes of cell injury and describes the differences between reversible and irreversible injury. Specific changes that characterize necrosis and apoptosis are discussed. Examples of cellular adaptations and morphologies of reversible and irreversible injury are provided.